Dahlgren Jovanna, Kriström Berit, Niklasson Aimon, Nierop Andreas F M, Rosberg Sten, Albertsson-Wikland Kerstin
Göteborg Pediatric Growth Research Center, Institute of Clinical Science, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden.
BMC Med Inform Decis Mak. 2007 Dec 12;7:40. doi: 10.1186/1472-6947-7-40.
Mathematical models can be used to predict individual growth responses to growth hormone (GH) therapy. The aim of this study was to construct and validate high-precision models to predict the growth response to GH treatment of short children, independent of their GH status, birth size and gestational age. As the GH doses are included, these models can be used to individualize treatment.
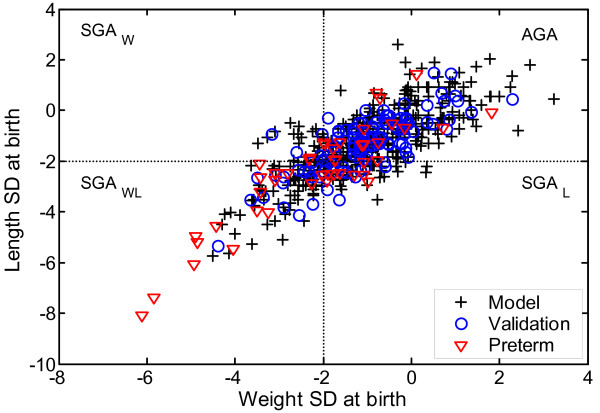
Growth data from 415 short prepubertal children were used to construct models for predicting the growth response during the first years of GH therapy. The performance of the models was validated with data from a separate cohort of 112 children using the same inclusion criteria.
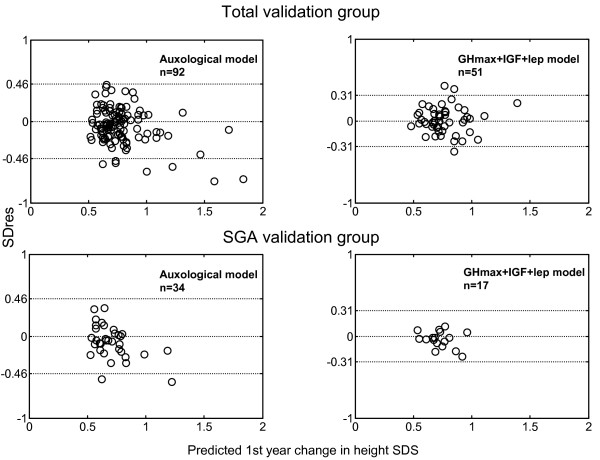
Using only auxological data, the model had a standard error of the residuals (SDres), of 0.23 SDS. The model was improved when endocrine data (GHmax profile, IGF-I and leptin) collected before starting GH treatment were included. Inclusion of these data resulted in a decrease of the SDres to 0.15 SDS (corresponding to 1.1 cm in a 3-year-old child and 1.6 cm in a 7-year old). Validation of these models with a separate cohort, showed similar SDres for both types of models. Preterm children were not included in the Model group, but predictions for this group were within the expected range.
These prediction models can with high accuracy be used to identify short children who will benefit from GH treatment. They are clinically useful as they are constructed using data from short children with a broad range of GH secretory status, birth size and gestational age.
数学模型可用于预测个体对生长激素(GH)治疗的生长反应。本研究的目的是构建并验证高精度模型,以预测身材矮小儿童对GH治疗的生长反应,而不考虑其GH状态、出生体重和胎龄。由于纳入了GH剂量,这些模型可用于个体化治疗。
使用415名青春期前身材矮小儿童的生长数据构建模型,以预测GH治疗最初几年的生长反应。使用来自112名儿童的另一队列的数据,采用相同的纳入标准对模型的性能进行验证。
仅使用体格学数据时,模型的残差标准差(SDres)为0.23 SDS。在纳入开始GH治疗前收集的内分泌数据(GHmax曲线、IGF-I和瘦素)后,模型得到改进。纳入这些数据后,SDres降至0.15 SDS(相当于3岁儿童为1.1 cm,7岁儿童为1.6 cm)。用另一队列对这些模型进行验证,结果显示两种模型的SDres相似。模型组未纳入早产儿,但该组的预测值在预期范围内。
这些预测模型可高精度地用于识别将从GH治疗中获益的身材矮小儿童。由于它们是使用来自具有广泛GH分泌状态、出生体重和胎龄的身材矮小儿童的数据构建的,因此在临床上具有实用性。