Poon Man-Chiu
Department of Medicine, University of Calgary, Alberta, Canada.
Vasc Health Risk Manag. 2007;3(5):655-64.
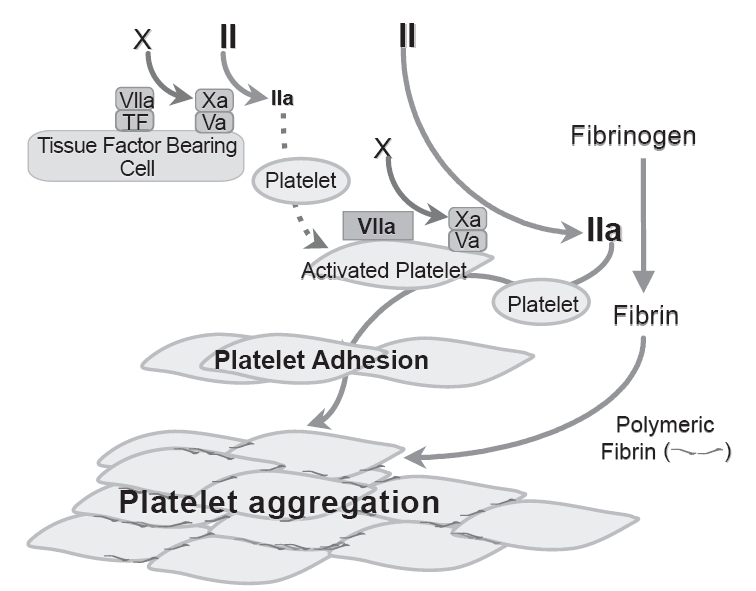
Glanzmann's thrombasthenia (GT) is a congenital qualitative platelet disorders due to the deficiency or defect of platelet membrane GPIIb/IIIa (integrin alpha(IIb)beta3). The standard treatment for bleeding is platelet transfusion but repeated transfusion may result in the development of anti-platelet antibodies (to HLA and/or GPlIbIIIa) rendering future platelet transfusion ineffective. Alternative effective agent(s) are needed. There are increasing reports documenting efficacy of high dose rFVIIa in GT patients with adverse events uncommon. The efficacy is supported by evidence that high concentration FVIIa binds to activated platelet surface and improves thrombin generation to enhance deposition (adhesion) and aggregation of platelets lacking GPIIb/IIIa. While there are increasing clinical experiences, evidence-based clinical data are not available. There is a need for more clinical studies, particularly clinical trials, to further assess the efficacy, safety (particularly thrombotic events) and optimal regimen ofrFVIIa in GT patients, either singly or in combination with other hemostatic agents such as platelet transfusion. In the absence of this data, for treatment of severe bleeding in GT patients with platelet antibodies and platelet refractoriness, rFVIIa at dose 90 microg/kg every 2 h for 3 or more doses could be considered. This more "optimal regimen" derived from a recent International Survey needs confirmation with larger studies. What the optimal regimen for surgical coverage is remains unresolved.
Glanzmann血小板无力症(GT)是一种先天性血小板质量异常疾病,由于血小板膜糖蛋白IIb/IIIa(整合素α(IIb)β3)缺乏或缺陷所致。出血的标准治疗方法是输注血小板,但反复输注可能导致抗血小板抗体(针对HLA和/或GPlIbIIIa)的产生,使未来的血小板输注无效。因此需要其他有效的药物。越来越多的报告记录了高剂量重组活化凝血因子VII(rFVIIa)在GT患者中的疗效,且不良事件并不常见。高浓度的FVIIa与活化的血小板表面结合并改善凝血酶生成,从而增强缺乏GPIIb/IIIa的血小板的沉积(黏附)和聚集,这一证据支持了其疗效。虽然临床经验不断增加,但基于证据的临床数据尚不可得。需要更多的临床研究,特别是临床试验,以进一步评估rFVIIa在GT患者中的疗效、安全性(特别是血栓形成事件)和最佳用药方案,无论是单独使用还是与其他止血药物如血小板输注联合使用。在缺乏这些数据的情况下,对于有血小板抗体和血小板输注无效的GT患者的严重出血治疗,可考虑每2小时给予90μg/kg的rFVIIa,共3剂或更多剂。这种来自最近一项国际调查的更“优化方案”需要通过更大规模的研究来证实。手术覆盖的最佳方案仍未解决。