Badero Olurotimi J, Salifu Moro O, Wasse Haimanot, Work Jack
Division of Nephrology, Emory University School of Medicine, Atlanta, GA, USA.
Am J Kidney Dis. 2008 Jan;51(1):93-8. doi: 10.1053/j.ajkd.2007.09.012.
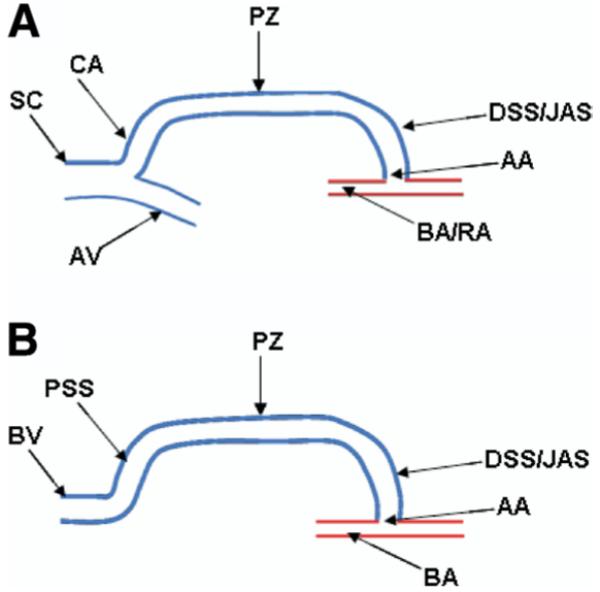
The segment of the vein mobilized for arterial anastomosis in the creation of an arteriovenous fistula (AVF) is the swing segment. This segment may experience turbulent flow and altered shear mechanical stress that result in stenosis. We sought to determine the frequency of stenotic lesions in the swing segment.
Case series.
SETTINGS & PARTICIPANTS: From January 31, 2003, to June 30, 2005, records of all patients referred to an outpatient hemodialysis vascular access center for AVF dysfunction were reviewed (n = 484). Of these, 278 patients had angiographically documented stenosis (any degree of luminal narrowing) on their first visit.
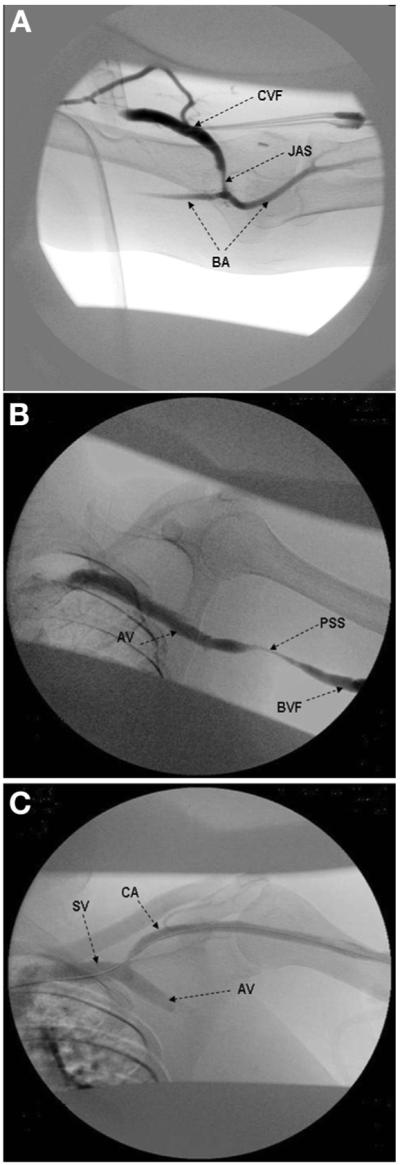
OUTCOMES & MEASUREMENTS: Distribution of stenoses in different segments of the AVF. Swing-segment stenoses were classified as proximal (outflow into axillary vein system), distal or juxta-anastomotic (adjacent to the anastomosis), and the cephalic arch.
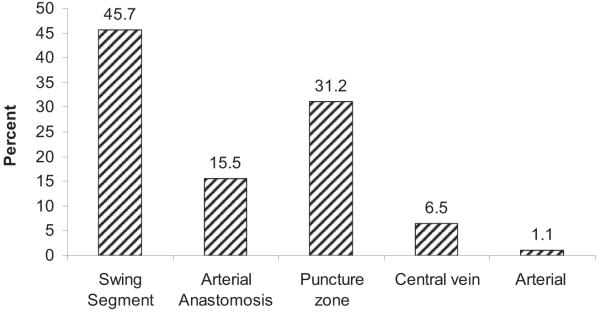
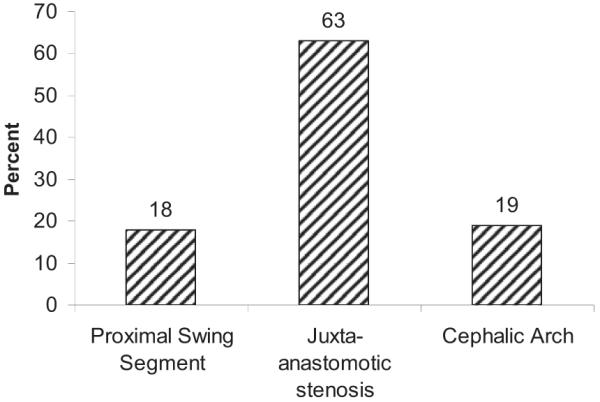
Overall prevalence of angiographically documented swing segment stenosis (proximal, distal or juxta-anastomotic, and cephalic arch) was 45.7% (127 of 278 patients), whereas the remaining stenoses (151 of 278 patients) were distributed among the puncture zone, arterial, arterial anastomosis, and central veins. The most frequent location of the swing-segment stenosis was juxta-anatomosis (63%; 80 of 127 patients), followed by cephalic arch (19%; 24 of 127 patients) and proximal swing segment (18%; 23 of 127 patients). The distribution of swing-segment stenosis (n = 127) was equivalent among the various fistulas (brachial-cephalic, 35.4%; radial-cephalic, 33.9%; and brachial-basilic, 30.7%). Eighty-three percent of swing-segment stenoses were significant (>50% luminal narrowing) and underwent percutaneous transluminal angioplasty, with a 93% success rate.
Retrospective nature of the study and potential selection bias.
In our population, swing-segment stenosis is the most common lesion in dysfunctional AVFs; juxta-anastomotic stenosis is the predominant lesion independent of fistula type. Whether the occurrence of swing-segment stenosis is caused by mobilization of the vein during surgery is not clear.
在动静脉内瘘(AVF)创建过程中用于动脉吻合而游离的静脉段为摆动段。该段可能会经历湍流和剪切机械应力改变,从而导致狭窄。我们试图确定摆动段狭窄病变的发生率。
病例系列研究。
从2003年1月31日至2005年6月30日,对所有转诊至门诊血液透析血管通路中心的因AVF功能障碍的患者记录进行回顾(n = 484)。其中,278例患者在首次就诊时经血管造影证实有狭窄(任何程度的管腔狭窄)。
AVF不同节段狭窄的分布情况。摆动段狭窄分为近端(流入腋静脉系统)、远端或吻合口旁(靠近吻合口)以及头静脉弓部。
经血管造影证实的摆动段狭窄(近端、远端或吻合口旁以及头静脉弓部)的总体发生率为45.7%(278例患者中的127例),而其余狭窄(278例患者中的151例)分布在穿刺区、动脉、动脉吻合口和中心静脉。摆动段狭窄最常见的部位是吻合口旁(63%;127例患者中的80例),其次是头静脉弓部(19%;127例患者中的24例)和近端摆动段(18%;127例患者中的23例)。摆动段狭窄(n = 127)在各种内瘘(肱动脉-头静脉,35.4%;桡动脉-头静脉,33.9%;肱动脉-贵要静脉,30.7%)中的分布情况相当。83%的摆动段狭窄较为严重(管腔狭窄>50%)并接受了经皮腔内血管成形术,成功率为93%。
研究的回顾性性质以及潜在的选择偏倚。
在我们的研究人群中,摆动段狭窄是功能障碍性AVF中最常见的病变;吻合口旁狭窄是主要病变,且与内瘘类型无关。摆动段狭窄的发生是否由手术中静脉的游离所致尚不清楚。