Gardner Andrew W, Montgomery Polly S, Parker Donald E
CMRI Metabolic Research Center, University of Oklahoma Health Sciences Center, 1122 NE 13th Street, Oklahoma City, OK 73117, USA.
J Vasc Surg. 2008 Jan;47(1):117-22. doi: 10.1016/j.jvs.2007.09.033.
We examined whether all-cause mortality was predicted by physical activity level in peripheral arterial disease (PAD) patients limited by intermittent claudication.
This retrospective, natural history follow-up study determined survival status of each patient. Patients with stable symptoms of intermittent claudication were evaluated in the Geriatrics, Research, Education, and Clinical Center at the Maryland Veterans Affairs Health Care System (MVAHCS) at Baltimore between 1994 and 2002, and were classified into a physically sedentary group (n = 299) or a physically active group (n =135), and followed in 2004 using the Social Security Death Index.
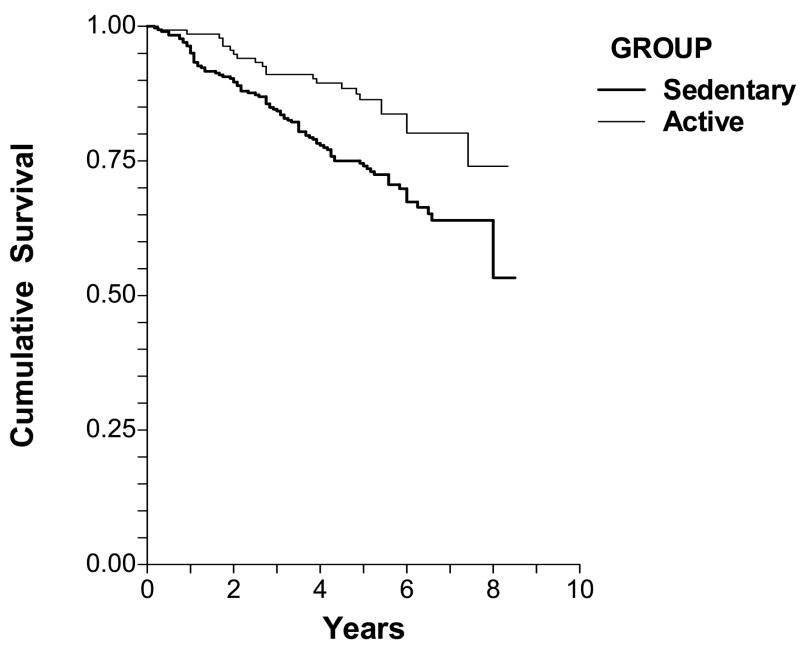
Median follow-up was 5.33 years (range = 0.25 to 8.33 years) for the physically active group, and 5.0 years (range = 0.17 to 8.5 years) for the sedentary group. At follow-up, 108 patients (24.9%) had died, consisting of 86 (28.8%) in the sedentary group and 22 (16.3%) in the active group. Unadjusted risk of mortality was lower (P = .005) in the physically active group (hazard ratio [HR] = 0.510, 95% CI = 0.319 to 0.816). In multivariate Cox proportional hazards analysis, age (HR = 1.045, 95% CI = 1.019 to 1.072, P < 0.001), body mass index (BMI) (HR = 0.943, 95% CI = 0.902 to 0.986, P = 0.009), ankle-brachial index (ABI) (HR = 0.202, 95% CI = 0.064 to 0.632, p = 0.006), and physical activity status (HR = 0.595, 95% CI = 0.370 to 0.955, P = .031) were predictors of mortality.
Patients limited by intermittent claudication who engage in any amount of weekly physical activity beyond light intensity at baseline have a lower mortality rate than their sedentary counterparts who perform either no physical activity or only light-intensity activities. The protective effect of physical activity persists even after adjusting for other predictors of mortality, which include age, ABI, and BMI.
我们研究了间歇性跛行限制的外周动脉疾病(PAD)患者的身体活动水平是否能预测全因死亡率。
这项回顾性自然病史随访研究确定了每位患者的生存状况。1994年至2002年期间,在巴尔的摩马里兰退伍军人事务医疗保健系统(MVAHCS)的老年医学、研究、教育和临床中心对症状稳定的间歇性跛行患者进行了评估,并将其分为身体久坐组(n = 299)或身体活跃组(n = 135),2004年使用社会保障死亡指数进行随访。
身体活跃组的中位随访时间为5.33年(范围 = 0.25至8.33年),久坐组为5.0年(范围 = 0.17至8.5年)。随访时,108例患者(24.9%)死亡,其中久坐组86例(28.8%),活跃组22例(16.3%)。身体活跃组的未调整死亡率较低(P = 0.005)(风险比[HR] = 0.510,95%置信区间 = 0.319至0.816)。在多变量Cox比例风险分析中,年龄(HR = 1.045,95%置信区间 = 1.019至1.072,P < 0.001)、体重指数(BMI)(HR = 0.943,95%置信区间 = 0.902至0.986,P = 0.009)、踝臂指数(ABI)(HR = 0.202,95%置信区间 = 0.064至0.632,P = 0.006)和身体活动状态(HR = 0.595,95%置信区间 = 0.370至0.955,P = 0.031)是死亡率的预测因素。
基线时每周进行任何超出轻度强度身体活动的间歇性跛行受限患者,其死亡率低于不进行身体活动或仅进行轻度强度活动的久坐同龄人。即使在调整了包括年龄、ABI和BMI在内的其他死亡率预测因素后,身体活动的保护作用仍然存在。