Oppegaard K S, Nesheim B-I, Istre O, Qvigstad E
Department of Gynaecology, Helse Finnmark, Klinikk Hammerfest, Hammerfest, Norway.
BJOG. 2008 Apr;115(5):663, e1-9. doi: 10.1111/j.1471-0528.2007.01628.x. Epub 2008 Jan 16.
To compare the impact of 1000 micrograms of self-administered vaginal misoprostol versus self-administered vaginal placebo at home on preoperative cervical ripening in both premenopausal and postmenopausal women before operative hysteroscopy.
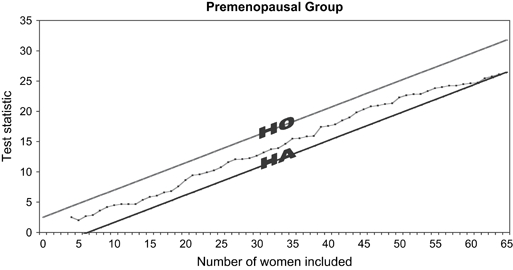
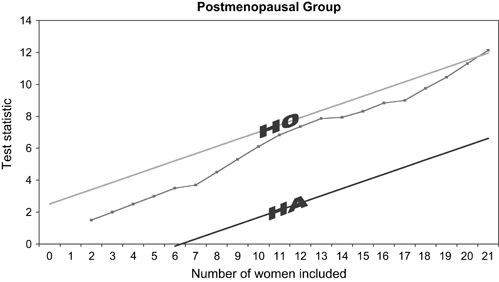
Two separate but identical parallel, randomised, double-blind, placebo-controlled sequential trials, one in premenopausal women and one in postmenopausal women. The boundaries for the sequential trials were calculated on the primary outcomes of a difference of cervical dilatation > or = 1 mm, with the assumption of a type 1 error of 0.05 and a power of 0.95.
Norwegian university teaching hospital.
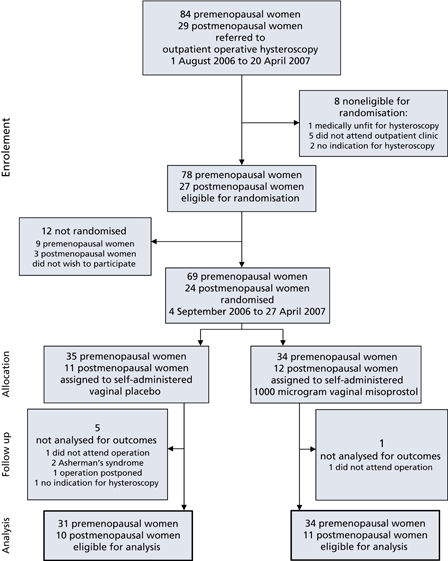
Eighty-six women referred to outpatient operative hysteroscopy.
The women were randomised to either 1000 micrograms of self-administered vaginal misoprostol or self-administered vaginal placebo the evening before outpatient operative hysteroscopy.
Preoperative cervical dilatation (primary outcome), number of women who achieve a preoperative cervical dilatation > or = 5 mm, acceptability, complications and adverse effects (secondary outcomes).
In premenopausal women, the mean cervical dilatation was 6.4 mm (SD 2.4) in the misoprostol group and 4.8 mm (SD 2.0) in the placebo group, the mean difference in cervical dilatation being 1.6 mm (95% CI 0.5-2.7). Among the premenopausal women receiving misoprostol, 88% achieved a cervical dilatation of > or = 5 mm compared with 65% in the placebo group. Twelve percent of the women who received misoprostol were difficult to dilate compared with 32% who received placebo. Dilatation was also quicker in the misoprostol group. Misoprostol had no effect on cervical ripening in postmenopausal women compared with placebo, and 43% of the women were difficult to dilate. The trials were terminated after analysis of 21 postmenopausal women and 65 premenopausal women after reaching a conclusion on the primary outcome with only 28% of the number of women needed in a fixed sample size trial. Three of 45 women who received misoprostol experienced severe lower abdominal pain, and there was an increased occurrence of light preoperative bleeding in the misoprostol group. Most women did not experience misoprostol-related adverse effects. The majority (83% of premenopausal and 76% of postmenopausal women) found self-administered vaginal misoprostol at home to be acceptable. There were two serious complications in the premenopausal misoprostol group: uterine perforation with subsequent peritonitis and heavy postoperative bleeding requiring blood transfusion, but these were not judged to be misoprostol related. Complications were otherwise comparatively minor and distributed equally between the two dosage groups.
One thousand micrograms of self-administered vaginal misoprostol 12 hours prior to operative hysteroscopy has a significant cervical ripening effect compared with placebo in premenopausal but not in postmenopausal women. Self-administered vaginal misoprostol of 1000 micrograms at home the evening before operative hysteroscopy is safe and highly acceptable, although a small proportion of women experienced severe lower abdominal pain. There is a risk of lower abdominal pain and light preoperative bleeding with this regimen, which is very cheap and easy to use.
比较术前在家自行阴道给予1000微克米索前列醇与自行阴道给予安慰剂对绝经前和绝经后妇女宫腔镜手术前宫颈成熟的影响。
两项独立但相同的平行、随机、双盲、安慰剂对照序贯试验,一项针对绝经前妇女,一项针对绝经后妇女。序贯试验的界限基于宫颈扩张差异≥1毫米的主要结局计算得出,假设Ⅰ类错误为0.05,检验效能为0.95。
挪威大学教学医院。
86名被转介至门诊进行宫腔镜手术的妇女。
这些妇女在门诊宫腔镜手术前一晚被随机分为自行阴道给予1000微克米索前列醇组或自行阴道给予安慰剂组。
术前宫颈扩张(主要结局)、术前宫颈扩张≥5毫米的妇女数量、可接受性、并发症和不良反应(次要结局)。
在绝经前妇女中,米索前列醇组的平均宫颈扩张为6.4毫米(标准差2.4),安慰剂组为4.8毫米(标准差2.0),宫颈扩张的平均差异为1.6毫米(95%可信区间0.5 - 2.7)。在接受米索前列醇的绝经前妇女中,88%的宫颈扩张≥5毫米,而安慰剂组为65%。接受米索前列醇的妇女中有12%难以扩张,而接受安慰剂的为32%。米索前列醇组的扩张也更快。与安慰剂相比,米索前列醇对绝经后妇女的宫颈成熟无影响,43%的妇女难以扩张。在对主要结局得出结论后,对21名绝经后妇女和65名绝经前妇女进行分析后试验终止,此时样本量仅为固定样本量试验所需妇女数量的28%。45名接受米索前列醇的妇女中有3名经历了严重的下腹痛,米索前列醇组术前轻度出血的发生率增加。大多数妇女未经历与米索前列醇相关的不良反应。大多数(绝经前妇女的83%和绝经后妇女的76%)认为在家自行阴道给予米索前列醇是可接受的。绝经前米索前列醇组有两项严重并发症:子宫穿孔继发腹膜炎和术后大出血需要输血,但这些未被判定与米索前列醇有关。其他并发症相对较轻,且在两个剂量组中分布均匀。
与安慰剂相比,术前12小时自行阴道给予1000微克米索前列醇对绝经前妇女有显著的宫颈成熟作用,但对绝经后妇女无此作用。手术前一晚在家自行阴道给予1000微克米索前列醇是安全且高度可接受的,尽管一小部分妇女经历了严重的下腹痛。这种方案存在下腹痛和术前轻度出血的风险,但其非常便宜且易于使用。