Acharya Munjal M, Hattiangady Bharathi, Shetty Ashok K
Medical Research and Surgery Services, Veterans Affairs Medical Center, Durham, NC 27705, USA.
Prog Neurobiol. 2008 Apr;84(4):363-404. doi: 10.1016/j.pneurobio.2007.10.010. Epub 2007 Dec 8.
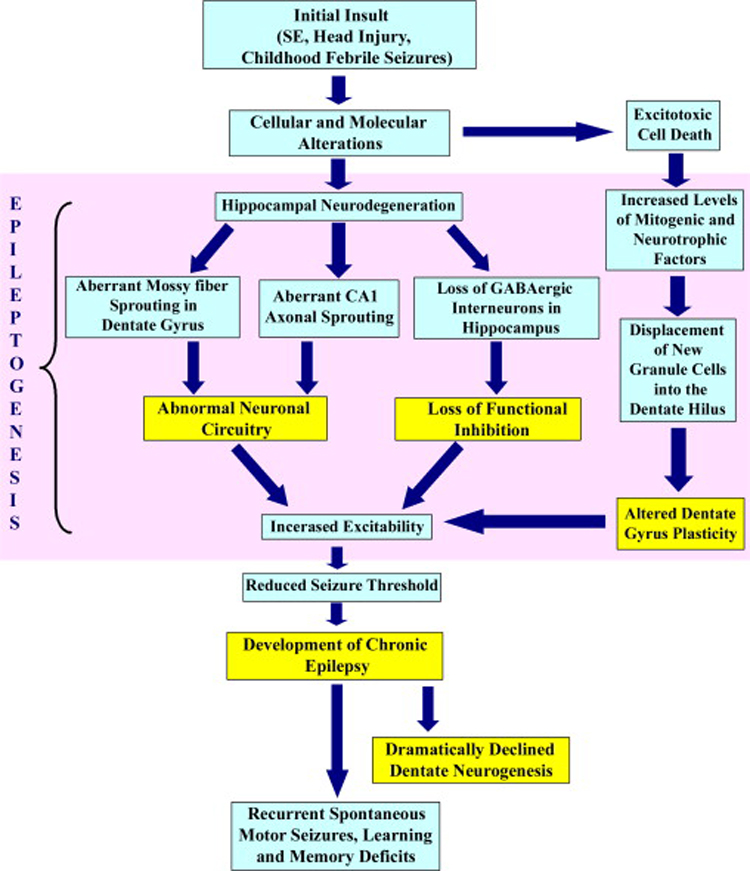
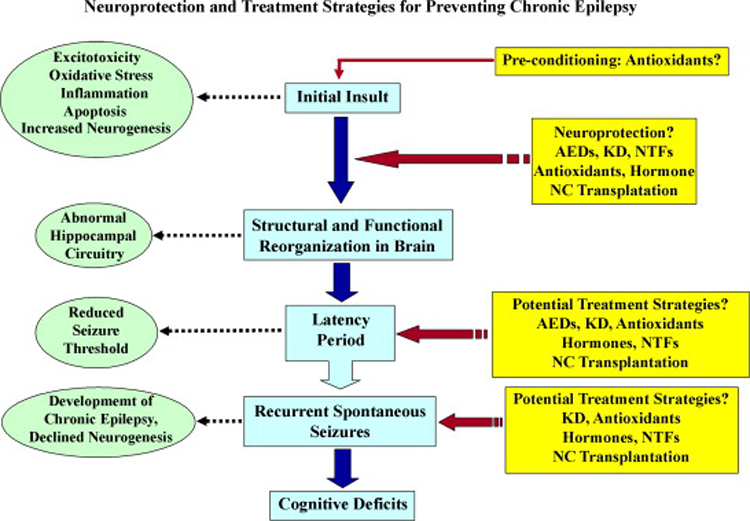
Neuroprotection is increasingly considered as a promising therapy for preventing and treating temporal lobe epilepsy (TLE). The development of chronic TLE, also termed as epileptogenesis, is a dynamic process. An initial precipitating injury (IPI) such as the status epilepticus (SE) leads to neurodegeneration, abnormal reorganization of the brain circuitry and a significant loss of functional inhibition. All of these changes likely contribute to the development of chronic epilepsy, characterized by spontaneous recurrent motor seizures (SRMS) and learning and memory deficits. The purpose of this review is to discuss the current state of knowledge pertaining to neuroprotection in epileptic conditions, and to highlight the efficacy of distinct neuroprotective strategies for preventing or treating chronic TLE. Although the administration of certain conventional and new generation anti-epileptic drugs is effective for primary neuroprotection such as reduced neurodegeneration after acute seizures or the SE, their competence for preventing the development of chronic epilepsy after an IPI is either unknown or not promising. On the other hand, alternative strategies such as the ketogenic diet therapy, administration of distinct neurotrophic factors, hormones or antioxidants seem useful for preventing and treating chronic TLE. However, long-term studies on the efficacy of these approaches introduced at different time-points after the SE or an IPI are lacking. Additionally, grafting of fetal hippocampal cells at early time-points after an IPI holds considerable promise for preventing TLE, though issues regarding availability of donor cells, ethical concerns, timing of grafting after SE, and durability of graft-mediated seizure suppression need to be resolved for further advances with this approach. Overall, from the studies performed so far, there is consensus that neuroprotective strategies need to be employed as quickly as possible after the onset of the SE or an IPI for considerable beneficial effects. Nevertheless, ideal strategies that are capable of facilitating repair and functional recovery of the brain after an IPI and preventing the evolution of IPI into chronic epilepsy are still hard to pin down.
神经保护越来越被认为是预防和治疗颞叶癫痫(TLE)的一种有前景的疗法。慢性TLE的发展,也称为癫痫发生,是一个动态过程。诸如癫痫持续状态(SE)之类的初始促发损伤(IPI)会导致神经变性、脑回路异常重组以及功能抑制的显著丧失。所有这些变化可能都有助于慢性癫痫的发展,其特征为自发性反复运动性癫痫发作(SRMS)以及学习和记忆缺陷。本综述的目的是讨论癫痫状态下神经保护的当前知识状态,并强调不同神经保护策略在预防或治疗慢性TLE方面的疗效。尽管某些传统和新一代抗癫痫药物的给药对于原发性神经保护是有效的,例如减少急性癫痫发作或SE后的神经变性,但其预防IPI后慢性癫痫发展的能力要么未知,要么前景不佳。另一方面,诸如生酮饮食疗法、给予不同的神经营养因子、激素或抗氧化剂等替代策略似乎对预防和治疗慢性TLE有用。然而,缺乏关于在SE或IPI后不同时间点引入这些方法的疗效的长期研究。此外,在IPI后早期移植胎儿海马细胞对于预防TLE具有很大的前景,尽管对于这种方法的进一步进展而言,供体细胞的可用性、伦理问题、SE后移植的时机以及移植介导的癫痫发作抑制的持久性等问题需要得到解决。总体而言,从迄今为止进行的研究来看,人们一致认为,在SE或IPI发作后应尽快采用神经保护策略以获得显著的有益效果。然而,能够促进IPI后脑的修复和功能恢复并防止IPI演变为慢性癫痫的理想策略仍然难以确定。