Pettifor John M
MRC Mineral Metabolism Research Unit, Department of Paediatrics, Chris Hani Baragwanath Hospital, University of the Witwatersrand, PO Bertsham 2013, Johannesburg, South Africa.
Eur J Pediatr. 2008 May;167(5):493-9. doi: 10.1007/s00431-007-0662-1. Epub 2008 Jan 24.
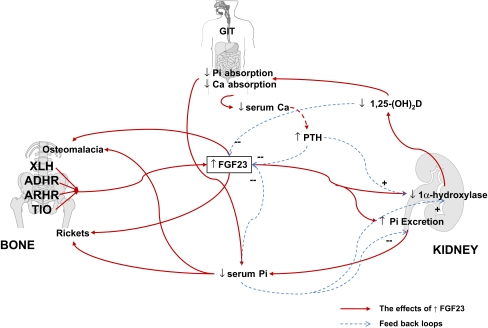
Although relatively uncommon individually, the various causes of hypophosphataemic rickets have provided an impetus for unravelling the mechanisms of phosphate homeostasis and bone mineralisation. Over the past 10 years, considerable advances have been made in establishing the gene mutations responsible for a number of the inherited causes and in understanding the mechanisms responsible for tumour-induced osteomalacia/rickets. The most exciting aspects of these discoveries have been the discovery of a whole new class of hormones or phosphatonins which are thought to control phosphate homoeostasis and 1 alpha-hydroxylase activity in the kidney, through a bone-kidney-intestinal tract axis. Although our understanding of the interrelationships is far from complete, it raises the possibilities of improved therapeutic agents in the long-term, and has resulted in improved diagnostic abilities in the short-term.
尽管各种导致低磷性佝偻病的病因单独来看相对不常见,但它们推动了对磷稳态和骨矿化机制的深入研究。在过去十年中,在确定多种遗传性病因所涉及的基因突变以及理解肿瘤诱导的骨软化症/佝偻病的发病机制方面取得了相当大的进展。这些发现中最令人兴奋的是发现了一类全新的激素或磷调节素,它们被认为通过骨-肾-肠道轴控制肾脏中的磷稳态和1α-羟化酶活性。尽管我们对它们之间相互关系的理解还远未完善,但从长远来看,这增加了开发更好治疗药物的可能性,并且在短期内提高了诊断能力。