Lerner Seth P, Tangen Catherine M, Sucharew Heidi, Wood David, Crawford E David
Scott Department of Urology, Baylor College of Medicine, Houston, TX 77030, USA.
Urol Oncol. 2009 Mar-Apr;27(2):155-9. doi: 10.1016/j.urolonc.2007.11.033. Epub 2008 Mar 4.
The Southwest Oncology Group conducted a randomized trial of induction bacillus Calmette-Guérin (BCG) with or without maintenance BCG. In these additional retrospective analyses, our goal was to evaluate the association of a complete response (CR) or remaining with no evidence of disease (NED) vs. no CR during induction therapy with subsequent survival after adjusting for other potential confounders. Among all patients randomized to maintenance treatment, we also wanted to identify combinations of baseline covariates in order to define prognostic groups for subsequent worsening-free survival.
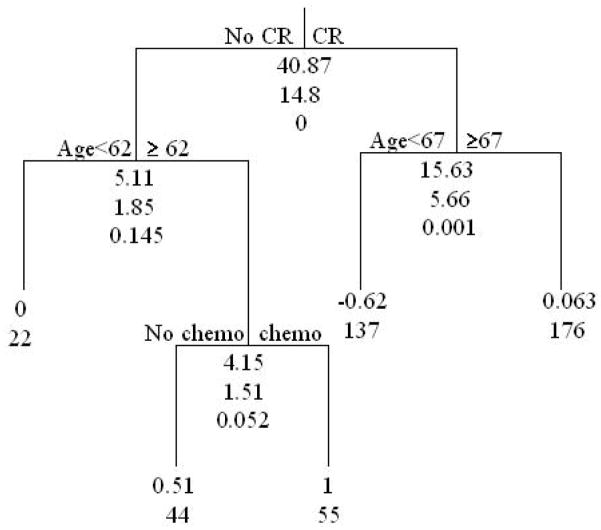
Outcome measures of worsening-free and overall survival were assessed using Kaplan Meier estimates and proportional hazards regression models. For the classification and regression tree (CART) analysis, 434 patients randomized to maintenance vs. no therapy with complete covariate information were included.
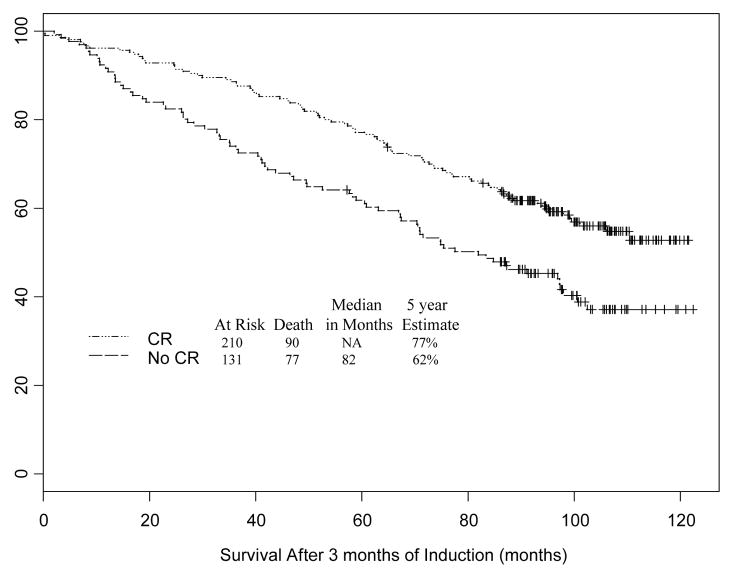
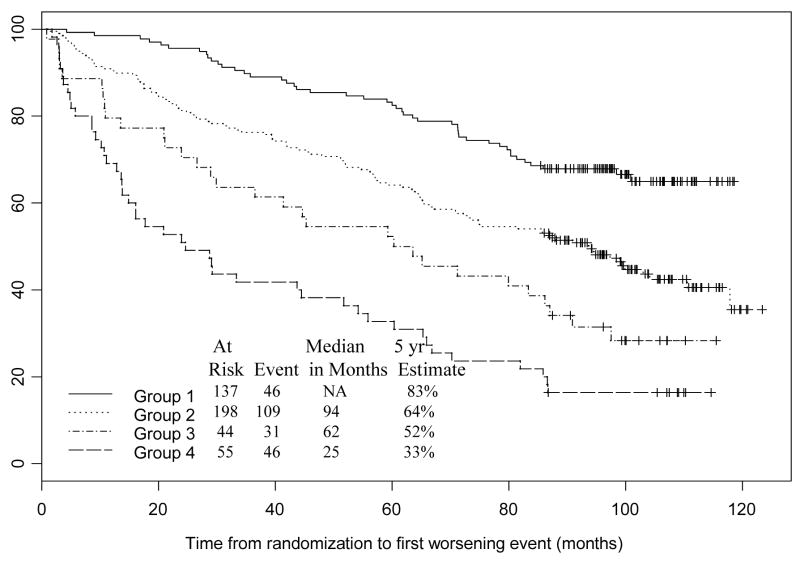
Of the 593 evaluable patients, 341 were not randomized to maintenance BCG. Patients who achieved a prior complete response during induction BCG had a 5-year survival probability of 77% compared with 62% for patients who did not [hazard ratio (HR) 0.60; 95% confidence interval (CI) 0.44, 0.81; P = 0.0008]. Prior CR retained significance when adjusted for age, gender, prior intravesical chemotherapy, and papillary disease versus CIS (HR = 0.63; 95% CI: 0.46, 0.86; P = 0.003). CART analysis identified 4 prognostic groups. Older patients (> or =62 years old) previously treated with intravesical chemotherapy who failed to achieve a CR had a 5-fold higher risk of a worsening event relative to those who are younger (<67 years old) and achieve a CR (HR = 5.09; 95% CI: 3.37, 7.68; P < 0.0001).
Failure to achieve a complete response after induction BCG is associated with a significant risk of a worsening event and death for patients with CIS or Ta or T1 bladder cancer at increased risk of recurrence.
西南肿瘤协作组开展了一项关于诱导使用卡介苗(BCG)并比较有无维持使用BCG的随机试验。在这些额外的回顾性分析中,我们的目标是在调整其他潜在混杂因素后,评估诱导治疗期间完全缓解(CR)或维持无疾病证据(NED)与未达到CR相比,对后续生存的影响。在所有随机接受维持治疗的患者中,我们还希望确定基线协变量的组合,以便为后续无恶化生存定义预后组。
使用Kaplan-Meier估计和比例风险回归模型评估无恶化生存和总生存的结局指标。对于分类与回归树(CART)分析,纳入了434例随机接受维持治疗与未接受治疗且具有完整协变量信息的患者。
在593例可评估患者中,341例未随机接受维持BCG治疗。诱导BCG治疗期间曾达到完全缓解的患者5年生存概率为77%,而未达到完全缓解的患者为62%[风险比(HR)0.60;95%置信区间(CI)0.44,0.81;P = 0.0008]。在调整年龄、性别、既往膀胱内化疗以及乳头状疾病与原位癌(CIS)后,既往CR仍具有显著性(HR = 0.63;95% CI:0.46,0.86;P = 0.003)。CART分析确定了4个预后组。既往接受膀胱内化疗且未达到CR的老年患者(≥62岁)发生恶化事件的风险比年轻患者(<67岁)且达到CR的患者高5倍(HR = 5.09;95% CI:3.37,7.68;P < 0.0001)。
对于复发风险增加的CIS或Ta或T1期膀胱癌患者,诱导BCG治疗后未达到完全缓解与发生恶化事件和死亡的显著风险相关。