Kamitani Rei, Tanaka Nobuyuki, Anno Tadatsugu, Murakami Tetsushi, Masuda Tsukasa, Yasumizu Yota, Takeda Toshikazu, Morita Shinya, Kosaka Takeo, Mikami Shuji, Matsumoto Kazuhiro, Oya Mototsugu
Department of Urology, Keio University School of Medicine, Tokyo, Japan.
Department of Diagnostic Pathology, Keio University Hospital, Tokyo, Japan.
Cancer Sci. 2024 Dec;115(12):3963-3972. doi: 10.1111/cas.16333. Epub 2024 Oct 11.
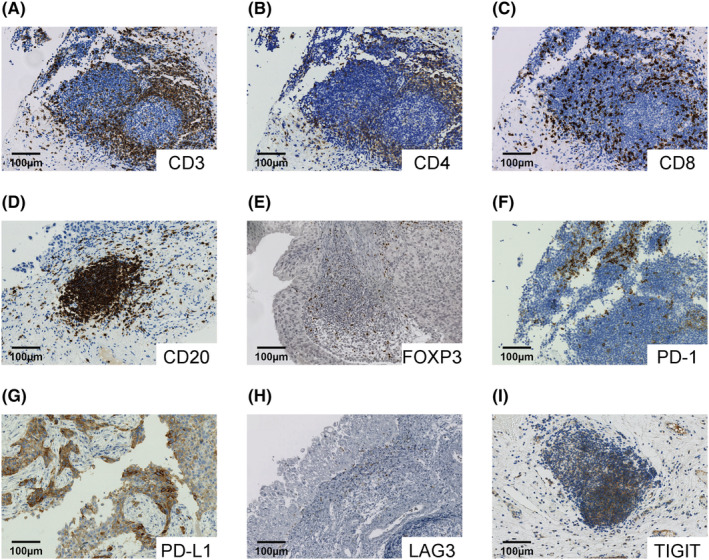
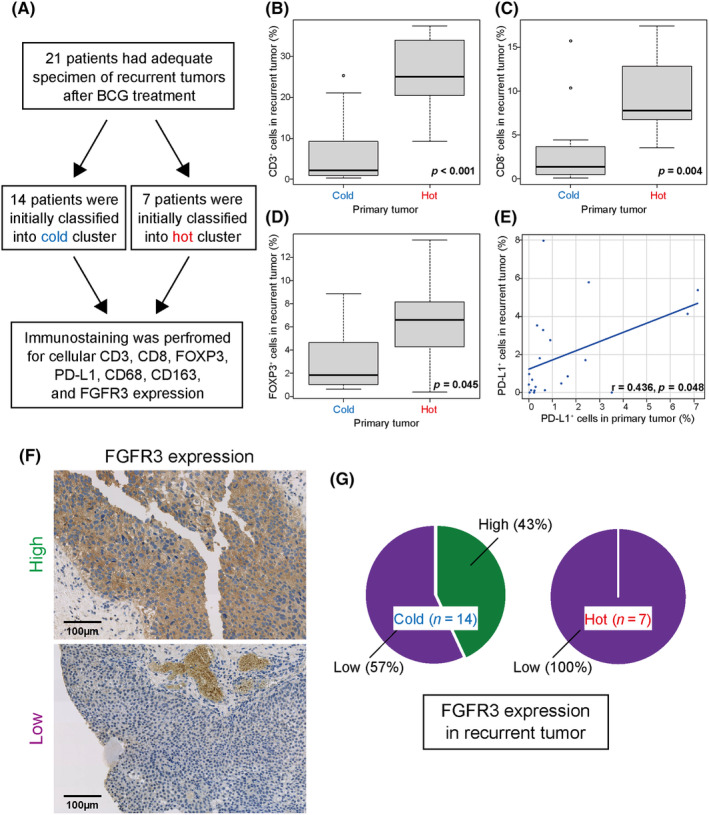
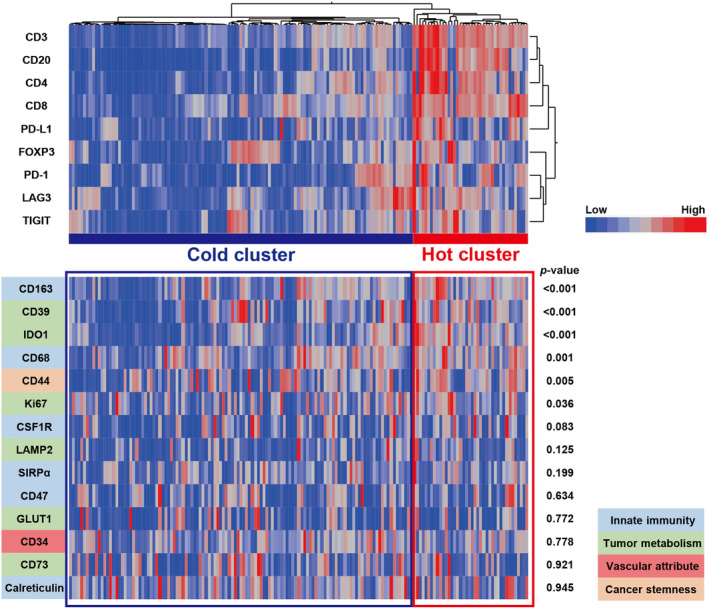
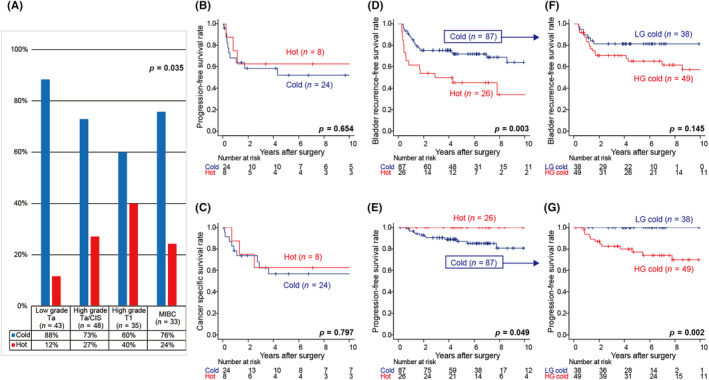
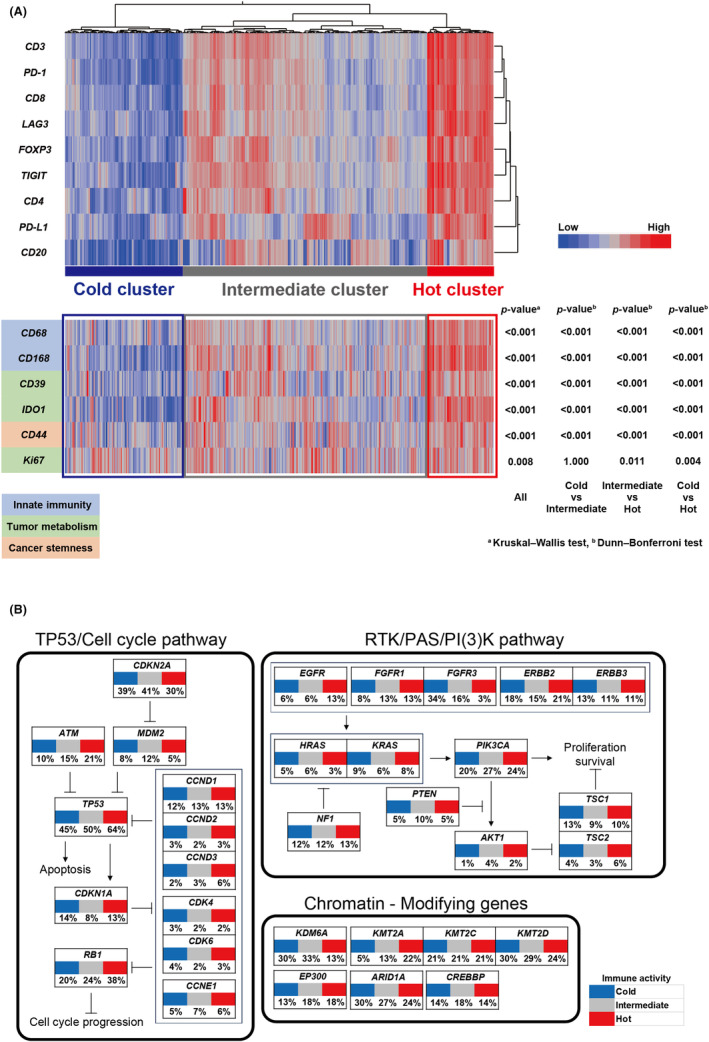
Agents that target PD-1 and PD-L1 have been developed in the treatment of bladder cancer (BC). However, the diversity of immune cell infiltration in non-muscle-invasive BC (NMIBC) and the dynamics of the microenvironment as it progresses to muscle-invasive/metastatic disease remains unknown. To assess tumor immune activity, hierarchical clustering was applied to 159 BC samples based on cellular positivity for the defined immune cellular markers (CD3/CD4/CD8/FOXP3/CD20/PD-1/PD-L1/LAG3/TIGIT), divided into two clusters. There was a "hot cluster" (25%) consisting of patients with a high expression of these markers and a "cold cluster" (75%) comprising those without. The expression of CD39, CD44, CD68, CD163, IDO1, and Ki67 was significantly higher in tumors in the hot cluster. Immunologically, high-grade T1 tumors were significantly hotter, whereas tumors that had progressed to muscle invasion turned cold. However, a certain number of high-grade NMIBC patients were in the cold cluster, and these patients had a significantly higher risk of disease progression. Using an externally available TCGA dataset, RB1 and TP53 alterations were more frequently observed in TCGA hot cluster; rather FGFR3, KDM6A, and KMT2A alterations were common in TCGA cold/intermediate cluster. Analyses of recurrent tumors after BCG therapy revealed that tumor immune activity was widely maintained before and after treatment, and high FGFR3 expression was detected after recurrence in tumors initially classified into the cold cluster. Collectively, we revealed the dynamics of the tumor microenvironment in BC as a whole and identified candidate molecules as therapeutic targets for recurrent NMIBC, e.g., after BCG therapy.
已开发出靶向程序性死亡受体 1(PD-1)和程序性死亡配体 1(PD-L1)的药物用于膀胱癌(BC)的治疗。然而,非肌层浸润性膀胱癌(NMIBC)中免疫细胞浸润的多样性以及其进展为肌层浸润性/转移性疾病时微环境的动态变化仍不清楚。为了评估肿瘤免疫活性,基于对定义的免疫细胞标志物(CD3/CD4/CD8/叉头框蛋白 P3(FOXP3)/CD20/PD-1/PD-L1/LAG3/T 细胞免疫球蛋白黏蛋白 3(TIGIT))的细胞阳性率,对 159 例 BC 样本进行层次聚类,分为两个簇。有一个“热簇”(25%),由这些标志物高表达的患者组成,还有一个“冷簇”(75%),由那些没有高表达的患者组成。热簇中的肿瘤中 CD39、CD44、CD68、CD163、吲哚胺 2,3-双加氧酶 1(IDO1)和 Ki67 的表达明显更高。在免疫方面,高级别 T1 肿瘤明显更“热”,而进展为肌层浸润的肿瘤则变“冷”。然而,一定数量的高级别 NMIBC 患者处于冷簇中,这些患者疾病进展的风险明显更高。使用外部可用的癌症基因组图谱(TCGA)数据集,视网膜母细胞瘤 1(RB1)和肿瘤蛋白 p53(TP53)改变在 TCGA 热簇中更频繁地观察到;相反,成纤维细胞生长因子受体 3(FGFR3)、赖氨酸(K)特异性去甲基化酶 6A(KDM6A)和赖氨酸甲基转移酶 2A(KMT2A)改变在 TCGA 冷/中间簇中很常见。卡介苗(BCG)治疗后复发性肿瘤的分析显示,肿瘤免疫活性在治疗前后广泛维持,并且在最初分类为冷簇的肿瘤复发后检测到高 FGFR3 表达。总体而言,我们揭示了 BC 中肿瘤微环境的动态变化,并确定了候选分子作为复发性 NMIBC(例如 BCG 治疗后)的治疗靶点。