Ruggenenti Piero, Iliev Ilian, Costa Grazia Maria, Parvanova Aneliya, Perna Annalisa, Giuliano Giovanni Antonio, Motterlini Nicola, Ene-Iordache Bogdan, Remuzzi Giuseppe
Clinical Research Center for Rare Diseases, Aldo & Cele Daccò, Mario Negri Institute for Pharmacological Research, Bergamo, Italy.
Diabetes Care. 2008 Aug;31(8):1629-34. doi: 10.2337/dc08-0371. Epub 2008 Apr 28.
In patients with type 2 diabetes, left ventricular hypertrophy (LVH) predicts cardiovascular events, and the prevention of LVH is cardioprotective. We sought to compare the effect of ACE versus non-ACE inhibitor therapy on incident electrocardiographic (ECG) evidence of LVH (ECG-LVH).
This prespecified study compared the incidence of ECG-LVH by Sokolow-Lyon and Cornell voltage criteria in 816 hypertensive type 2 diabetic patients of the Bergamo Nephrologic Diabetes Complications Trial (BENEDICT), who had no ECG-LVH at baseline and were randomly assigned to at least 3 years of blinded ACE inhibition with trandolapril (2 mg/day) or to non-ACE inhibitor therapy. Treatment was titrated to systolic/diastolic blood pressure <130/80 mmHg. ECG readings were centralized and blinded to treatment.
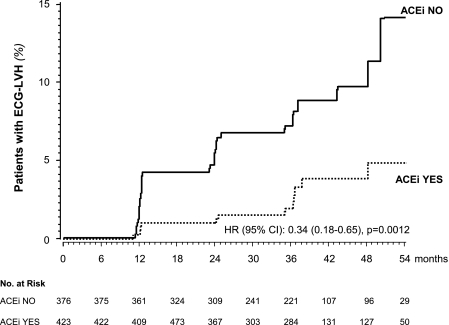
Baseline characteristics of the two groups were similar. Over a median (interquartile range) follow-up of 36 (24-48) months, 13 of the 423 patients (3.1%) receiving trandolapril compared with 31 of the 376 patients (8.2%) receiving non-ACE inhibitor therapy developed ECG-LVH (hazard ratio [HR] 0.34 [95% CI 0.18-0.65], P = 0.0012 unadjusted, and 0.35 [0.18-0.68], P = 0.0018 adjusted for predefined baseline covariates). The HR was significant even after adjustment for follow-up blood pressure and blood pressure reduction versus baseline. Compared with baseline, both Sokolow-Lyon and Cornell voltages significantly decreased with trandolapril but did not change with non-ACE inhibitor therapy.
ACE inhibition has a specific protective effect against the development of ECG-LVH that is additional to its blood pressure-lowering effect. Because ECG-LVH is a strong cardiovascular risk factor in people with hypertension and diabetes, early ACE inhibition may be cardioprotective in this population.
在2型糖尿病患者中,左心室肥厚(LVH)可预测心血管事件,预防LVH具有心脏保护作用。我们旨在比较ACE抑制剂与非ACE抑制剂治疗对新发心电图(ECG)左心室肥厚证据(ECG-LVH)的影响。
这项预先设定的研究比较了贝加莫肾脏糖尿病并发症试验(BENEDICT)中816例高血压2型糖尿病患者按Sokolow-Lyon和Cornell电压标准诊断的ECG-LVH发生率,这些患者基线时无ECG-LVH,被随机分配接受至少3年的盲法培哚普利(2 mg/天)ACE抑制治疗或非ACE抑制剂治疗。治疗调整至收缩压/舒张压<130/80 mmHg。ECG读数进行集中处理且对治疗方案设盲。
两组的基线特征相似。在中位(四分位间距)36(24 - 48)个月的随访中,423例接受培哚普利治疗的患者中有13例(3.1%)发生ECG-LVH,而376例接受非ACE抑制剂治疗的患者中有31例(8.2%)发生ECG-LVH(风险比[HR] 0.34 [95% CI 0.18 - 0.65],未校正P = 0.0012,校正预先定义的基线协变量后为0.35 [0.18 - 0.68],P = 0.0018)。即使在对随访血压以及与基线相比的血压降低情况进行校正后,HR仍具有显著性。与基线相比,培哚普利治疗后Sokolow-Lyon和Cornell电压均显著降低,而非ACE抑制剂治疗后未发生变化。
ACE抑制对ECG-LVH的发生具有特定的保护作用,这一作用独立于其降压作用。由于ECG-LVH是高血压和糖尿病患者的一个强大心血管危险因素,早期ACE抑制可能对该人群具有心脏保护作用。