De Cosmo Salvatore, Motterlini Nicola, Prudente Sabrina, Pellegrini Fabio, Trevisan Roberto, Bossi Antonio, Remuzzi Giuseppe, Trischitta Vincenzo, Ruggenenti Piero
Unit of Endocrinology, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy.
Diabetes. 2009 Dec;58(12):2920-9. doi: 10.2337/db09-0407. Epub 2009 Aug 31.
Cross-sectional studies found less microalbuminuria in type 2 diabetic patients with the Ala12 allele of the peroxisome proliferator-activated receptor-gamma2 (PPAR-gamma2) Pro12Ala polymorphism. We prospectively evaluated the association between Pro12Ala polymorphism (rs1801282) and new-onset microalbuminuria.
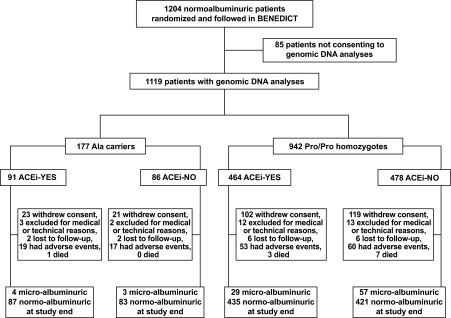
Pro12Ala polymorphism was genotyped by TaqMan-based assay in genomic DNA of 1,119 consenting patients from BErgamo NEphrologic DIabetic Complications Trial (BENEDICT)-a prospective, randomized trial evaluating ACE inhibition effect on new-onset microalbuminuria (albuminuria 20-200 microg/min in at least two of three consecutive overnight urine collections in two consecutive visits) in hypertensive type 2 diabetes with albuminuria <20 microg/min at inclusion.
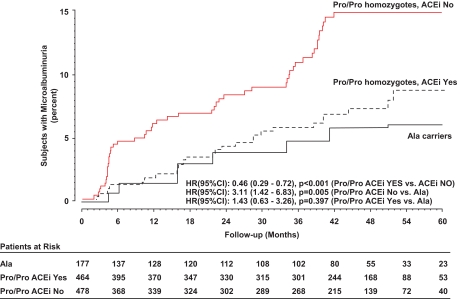
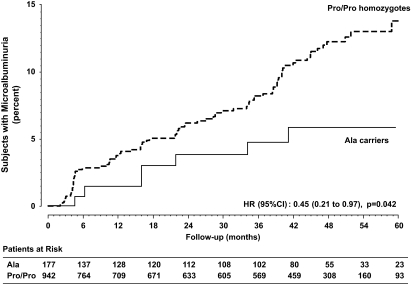
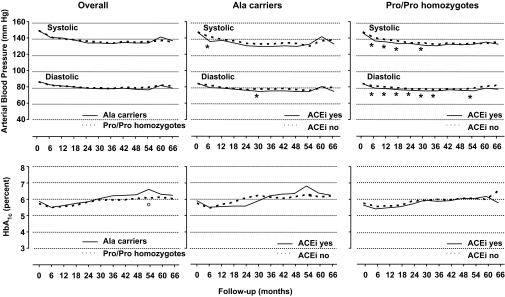
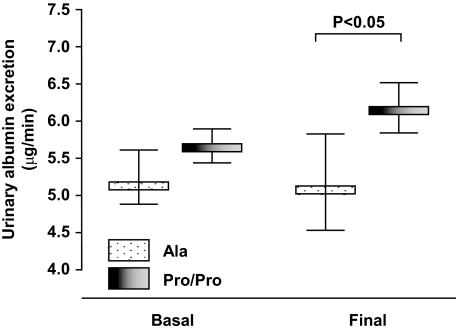
Baseline characteristics of Ala (Ala/Ala or Ala/Pro) carriers and Pro/Pro homozygotes were similar, with a nonsignificant trend to lower albuminuria (P = 0.1107) in the 177 Ala carriers. Over a median (interquartile range) of 44.0 (17.1-51.9) months, 7 (4%) Ala carriers and 86 (9.1%) Pro/Pro homozygotes developed microalbuminuria (hazard ratio [HR] 0.45 [95% CI 0.21-0.97]; P = 0.042). Final albuminuria was significantly lower in Ala carriers than Pro/Pro homozygotes (7.3 +/- 9.1 vs. 10.5 +/- 24.9 microg/min, respectively), even after adjustment for baseline albuminuria (P = 0.048). Baseline and follow-up blood pressure and metabolic control were similar in both groups. Incidence of microalbuminuria was significantly decreased by ACE versus non-ACE inhibitor therapy in Pro/Pro homozygotes (6.3 vs. 11.9%, respectively, HR 0.46 [0.29-0.72]; P < 0.001).
In type 2 diabetes, the Ala allele protects from worsening albuminuria and new-onset microalbuminuria, and ACE inhibition blunts the excess risk of microalbuminuria associated with the Pro/Pro genotype. Evaluating Pro12Ala polymorphism may help identifying patients at risk who may benefit the most from early renoprotective therapy.
横断面研究发现,过氧化物酶体增殖物激活受体γ2(PPAR-γ2)Pro12Ala多态性的Ala12等位基因在2型糖尿病患者中微量白蛋白尿较少。我们前瞻性评估了Pro12Ala多态性(rs1801282)与新发微量白蛋白尿之间的关联。
通过基于TaqMan的检测方法对来自贝加莫肾病糖尿病并发症试验(BENEDICT)的1119名同意参与研究的患者的基因组DNA进行Pro12Ala多态性基因分型。BENEDICT是一项前瞻性随机试验,评估ACE抑制对新发微量白蛋白尿(在连续两次就诊中至少三次连续夜间尿液收集中有两次白蛋白尿为20 - 200微克/分钟)的影响,纳入时高血压2型糖尿病患者白蛋白尿<20微克/分钟。
Ala(Ala/Ala或Ala/Pro)携带者和Pro/Pro纯合子的基线特征相似,177名Ala携带者中白蛋白尿有降低趋势但无统计学意义(P = 0.1107)。在中位(四分位间距)44.0(17.1 - 51.9)个月期间,7名(4%)Ala携带者和86名(9.1%)Pro/Pro纯合子出现微量白蛋白尿(风险比[HR] 0.45 [95% CI 0.21 - 0.97];P = 0.042)。即使在调整基线白蛋白尿后,Ala携带者的最终白蛋白尿仍显著低于Pro/Pro纯合子(分别为7.3±9.1与10.5±24.9微克/分钟,P = 0.048)。两组的基线和随访血压及代谢控制情况相似。在Pro/Pro纯合子中,ACE抑制剂治疗组与非ACE抑制剂治疗组相比,微量白蛋白尿的发生率显著降低(分别为6.3%与11.9%,HR 0.46 [0.29 - 0.72];P < 0.001)。
在2型糖尿病中,Ala等位基因可预防白蛋白尿恶化和新发微量白蛋白尿,且ACE抑制可降低与Pro/Pro基因型相关的微量白蛋白尿额外风险。评估Pro12Ala多态性可能有助于识别可能从早期肾脏保护治疗中获益最大的高危患者。