Tan Michael, Menzies Dick, Schwartzman Kevin
Respiratory Epidemiology Unit, Montreal Chest Institute, 3650 St, Urbain St,, Montreal, Quebec, H2X 2P4, Canada.
BMC Public Health. 2008 Jun 5;8:201. doi: 10.1186/1471-2458-8-201.
Travelers to countries with high tuberculosis incidence can acquire infection during travel. We sought to compare four screening interventions for travelers from low-incidence countries, who visit countries with varying tuberculosis incidence.
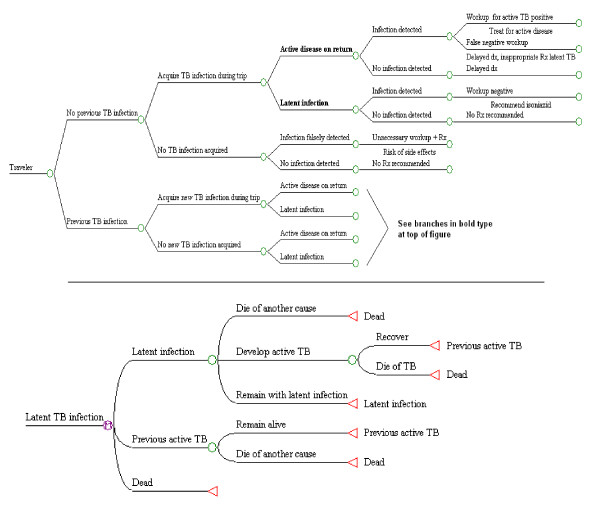
Decision analysis model: We considered hypothetical cohorts of 1,000 travelers, 21 years old, visiting Mexico, the Dominican Republic, or Haiti for three months. Travelers departed from and returned to the United States or Canada; they were born in the United States, Canada, or the destination countries. The time horizon was 20 years, with 3% annual discounting of future costs and outcomes. The analysis was conducted from the health care system perspective. Screening involved tuberculin skin testing (post-travel in three strategies, with baseline pre-travel tests in two), or chest radiography post-travel (one strategy). Returning travelers with tuberculin conversion (one strategy) or other evidence of latent tuberculosis (three strategies) were offered treatment. The main outcome was cost (in 2005 US dollars) per tuberculosis case prevented.
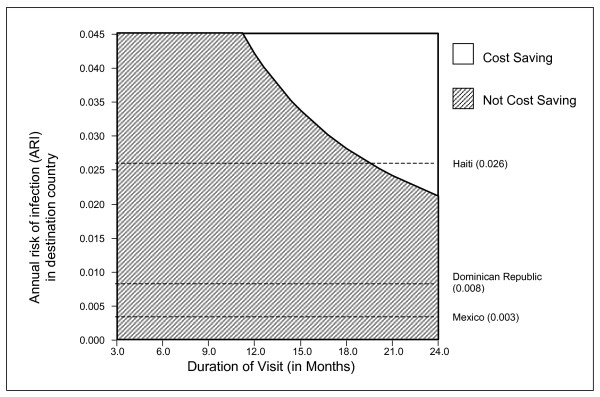
For all travelers, a single post-trip tuberculin test was most cost-effective. The associated cost estimate per case prevented ranged from $21,406 for Haitian-born travelers to Haiti, to $161,196 for US-born travelers to Mexico. In all sensitivity analyses, the single post-trip tuberculin test remained most cost-effective. For US-born travelers to Haiti, this strategy was associated with cost savings for trips over 22 months. Screening was more cost-effective with increasing trip duration and infection risk, and less so with poorer treatment adherence.
A single post-trip tuberculin skin test was the most cost-effective strategy considered, for travelers from the United States or Canada. The analysis did not evaluate the use of interferon-gamma release assays, which would be most relevant for travelers who received BCG vaccination after infancy, as in many European countries. Screening decisions should reflect duration of travel, tuberculosis incidence, and commitment to treat latent infection.
前往结核病高发国家的旅行者在旅行期间可能会感染结核菌。我们试图比较四种针对来自低发病率国家、前往结核病发病率各异国家的旅行者的筛查干预措施。
决策分析模型:我们考虑了1000名21岁旅行者的假设队列,他们前往墨西哥、多米尼加共和国或海地旅行三个月。旅行者从美国或加拿大出发并返回;他们出生在美国、加拿大或目的地国家。时间跨度为20年,未来成本和结果按每年3%进行贴现。分析是从医疗保健系统的角度进行的。筛查包括结核菌素皮肤试验(三种策略为旅行后进行,两种策略为旅行前进行基线检测),或旅行后胸部X光检查(一种策略)。结核菌素试验结果呈阳转的回国旅行者(一种策略)或其他潜伏性结核病证据的旅行者(三种策略)接受治疗。主要结果是预防每例结核病的成本(以2005年美元计)。
对于所有旅行者,单次旅行后结核菌素试验最具成本效益。预防每例病例的相关成本估计范围从出生在海地前往海地的旅行者的21406美元,到出生在美国前往墨西哥的旅行者的161196美元。在所有敏感性分析中,单次旅行后结核菌素试验仍然最具成本效益。对于出生在美国前往海地的旅行者,这种策略与超过22个月旅行的成本节省相关。随着旅行时间和感染风险的增加,筛查更具成本效益,而治疗依从性较差时则不然。
对于来自美国或加拿大的旅行者,单次旅行后结核菌素皮肤试验是所考虑的最具成本效益的策略。该分析未评估干扰素-γ释放试验的使用,而这对于许多欧洲国家中婴儿期后接种卡介苗的旅行者最为相关。筛查决策应反映旅行时间、结核病发病率以及治疗潜伏感染的意愿。