Lucchinetti C F, Gavrilova R H, Metz I, Parisi J E, Scheithauer B W, Weigand S, Thomsen K, Mandrekar J, Altintas A, Erickson B J, König F, Giannini C, Lassmann H, Linbo L, Pittock S J, Brück W
Department of Neurology, College of Medicine, Mayo Clinic, 200 First St SW, Rochester, MN 55905, USA.
Brain. 2008 Jul;131(Pt 7):1759-75. doi: 10.1093/brain/awn098. Epub 2008 Jun 5.
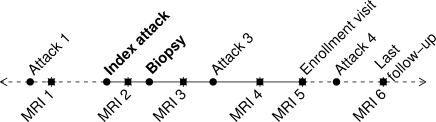
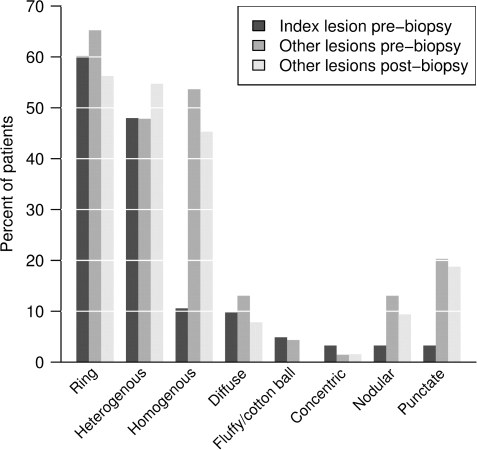
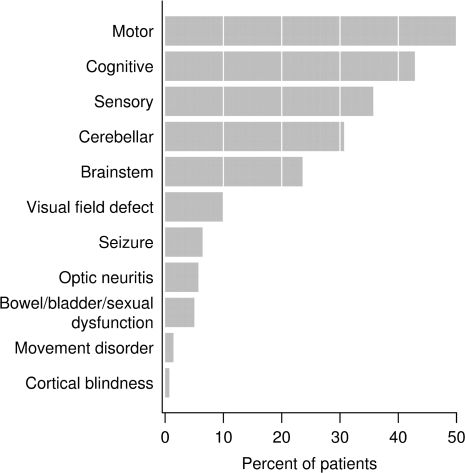
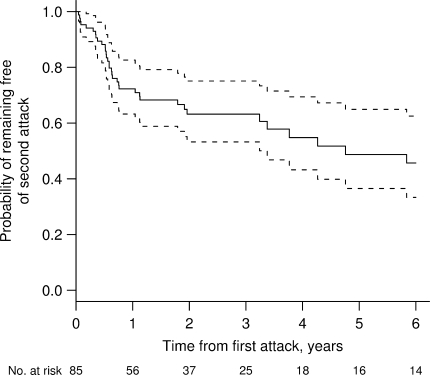
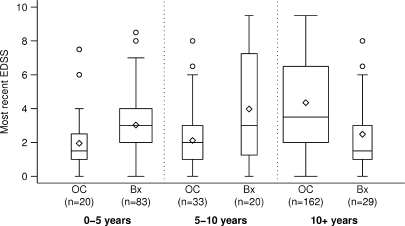
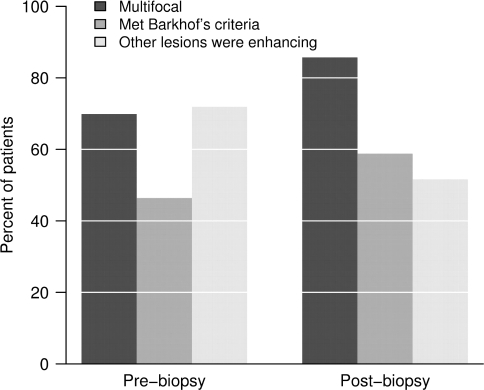
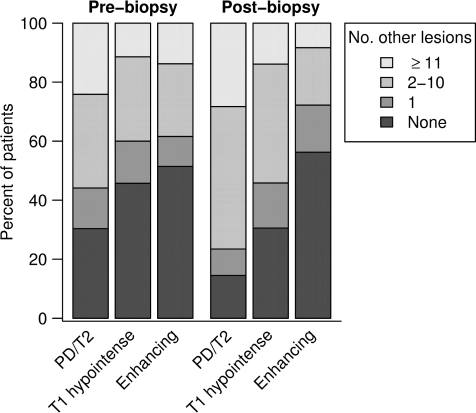
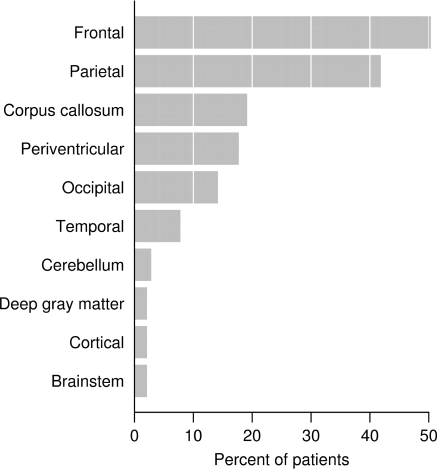
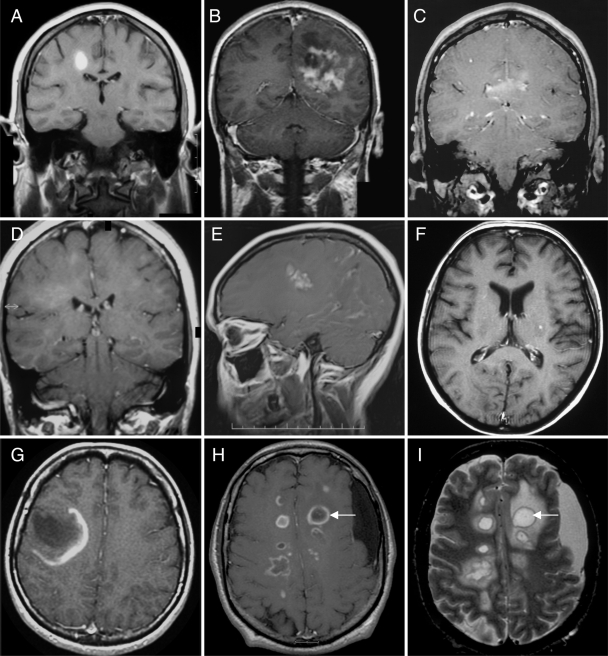
Atypical imaging features of multiple sclerosis lesions include size >2 cm, mass effect, oedema and/or ring enhancement. This constellation is often referred to as 'tumefactive multiple sclerosis'. Previous series emphasize their unifocal and clinically isolated nature, however, evolution of these lesions is not well defined. Biopsy may be required for diagnosis. We describe clinical and radiographic features in 168 patients with biopsy confirmed CNS inflammatory demyelinating disease (IDD). Lesions were analysed on pre- and post-biopsy magnetic resonance imaging (MRI) for location, size, mass effect/oedema, enhancement, multifocality and fulfilment of Barkhof criteria. Clinical data were correlated to MRI. Female to male ratio was 1.2 : 1, median age at onset, 37 years, duration between symptom onset and biopsy, 7.1 weeks and total disease duration, 3.9 years. Clinical course prior to biopsy was a first neurological event in 61%, relapsing-remitting in 29% and progressive in 4%. Presentations were typically polysymptomatic, with motor, cognitive and sensory symptoms predominating. Aphasia, agnosia, seizures and visual field defects were observed. At follow-up, 70% developed definite multiple sclerosis, and 14% had an isolated demyelinating syndrome. Median time to second attack was 4.8 years, and median EDSS at follow-up was 3.0. Multiple lesions were present in 70% on pre-biopsy MRI, and in 83% by last MRI, with Barkhof criteria fulfilled in 46% prior to biopsy and 55% by follow-up. Only 17% of cases remained unifocal. Median largest lesion size on T2-weighted images was 4 cm (range 0.5-12), with a discernible size of 2.1 cm (range 0.5-7.5). Biopsied lesions demonstrated mass effect in 45% and oedema in 77%. A strong association was found between lesion size, and presence of mass effect and/or oedema (P < 0.001). Ring enhancement was frequent. Most tumefactive features did not correlate with gender, course or diagnosis. Although lesion size >5 cm was associated with a slightly higher EDSS at last follow-up, long-term prognosis in patients with disease duration >10 years was better (EDSS 1.5) compared with a population-based multiple sclerosis cohort matched for disease duration (EDSS 3.5; P < 0.001). Given the retrospective nature of the study, the precise reason for biopsy could not always be determined. This study underscores the diagnostically challenging nature of CNS IDDs that present with atypical clinical or radiographic features. Most have multifocal disease at onset, and develop RRMS by follow-up. Although increased awareness of this broad spectrum may obviate need for biopsy in many circumstances, an important role for diagnostic brain biopsy may be required in some cases.
多发性硬化病变的非典型影像学特征包括大小>2 cm、占位效应、水肿和/或环形强化。这一组合通常被称为“瘤样多发性硬化”。既往系列研究强调其单灶性和临床孤立性,然而,这些病变的演变情况尚不明确。诊断可能需要活检。我们描述了168例经活检证实为中枢神经系统炎性脱髓鞘疾病(IDD)患者的临床和影像学特征。在活检前和活检后的磁共振成像(MRI)上分析病变的位置、大小、占位效应/水肿、强化、多灶性以及是否符合巴霍夫标准。将临床数据与MRI相关联。女性与男性比例为1.2:1,发病年龄中位数为37岁,症状出现至活检的持续时间为7.1周,疾病总持续时间为3.9年。活检前的临床病程中,61%为首次神经系统事件,29%为复发缓解型,4%为进展型。临床表现通常为多症状,以运动、认知和感觉症状为主。观察到失语、失认、癫痫发作和视野缺损。在随访中,70%发展为明确的多发性硬化,14%患有孤立性脱髓鞘综合征。第二次发作的中位时间为4.8年,随访时的扩展残疾状态量表(EDSS)中位数为3.0。活检前MRI显示70%存在多个病变,最后一次MRI显示83%存在多个病变,活检前46%符合巴霍夫标准,随访时55%符合。仅17%的病例仍为单灶性。T2加权图像上最大病变的中位大小为4 cm(范围0.5 - 12 cm),可辨别的大小为2.1 cm(范围0.5 - 7.5 cm)。活检的病变中45%显示占位效应,77%显示水肿。发现病变大小与占位效应和/或水肿的存在之间存在强关联(P < 0.)。环形强化很常见。大多数瘤样特征与性别、病程或诊断无关。尽管病变大小>5 cm与最后一次随访时略高的EDSS相关,但病程>10年患者的长期预后(EDSS 1.5)优于与之匹配的基于人群的多发性硬化队列(EDSS 3.5;P < 0.001)。鉴于该研究的回顾性性质,活检的确切原因并非总能确定。这项研究强调了具有非典型临床或影像学特征的中枢神经系统IDD在诊断上具有挑战性。大多数患者起病时为多灶性疾病,随访时发展为复发缓解型多发性硬化。尽管提高对这一广泛谱系的认识可能在许多情况下避免活检的必要性,但在某些情况下诊断性脑活检可能仍起着重要作用。