School of Medicine, Menzies Health Institute Queensland, Gold Coast Campus, Griffith University, Gold Coast, QLD, 4222, Australia.
Department of Neurology, Gold Coast University Hospital, Southport, QLD, 4215, Australia.
J Neurol. 2024 Aug;271(8):5275-5289. doi: 10.1007/s00415-024-12349-6. Epub 2024 Jun 11.
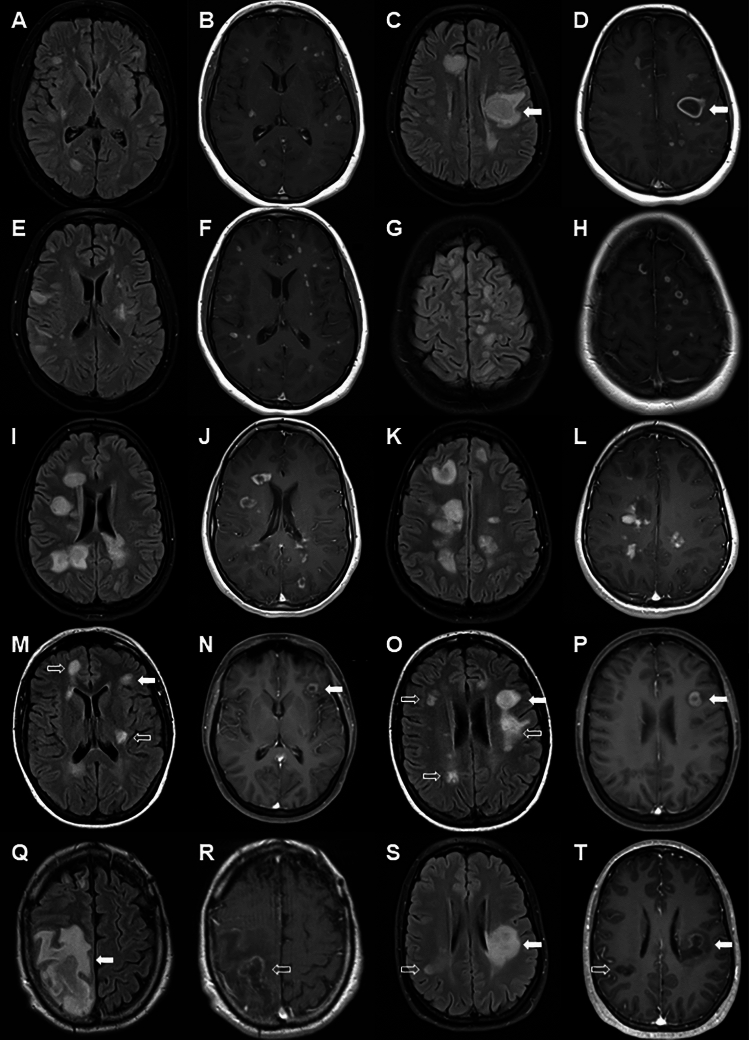
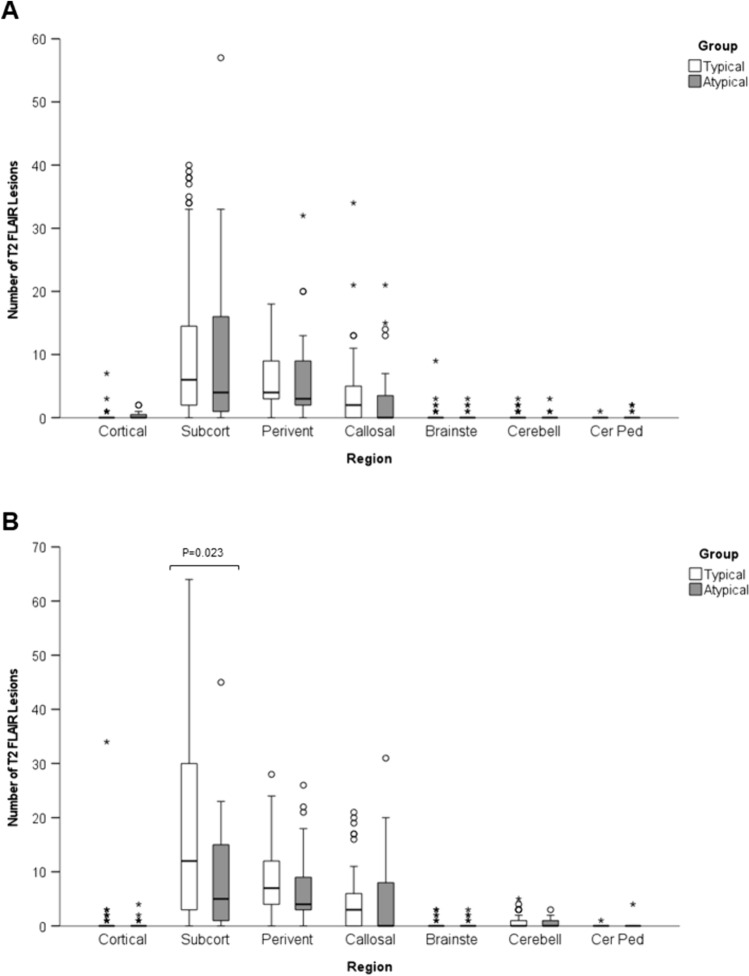
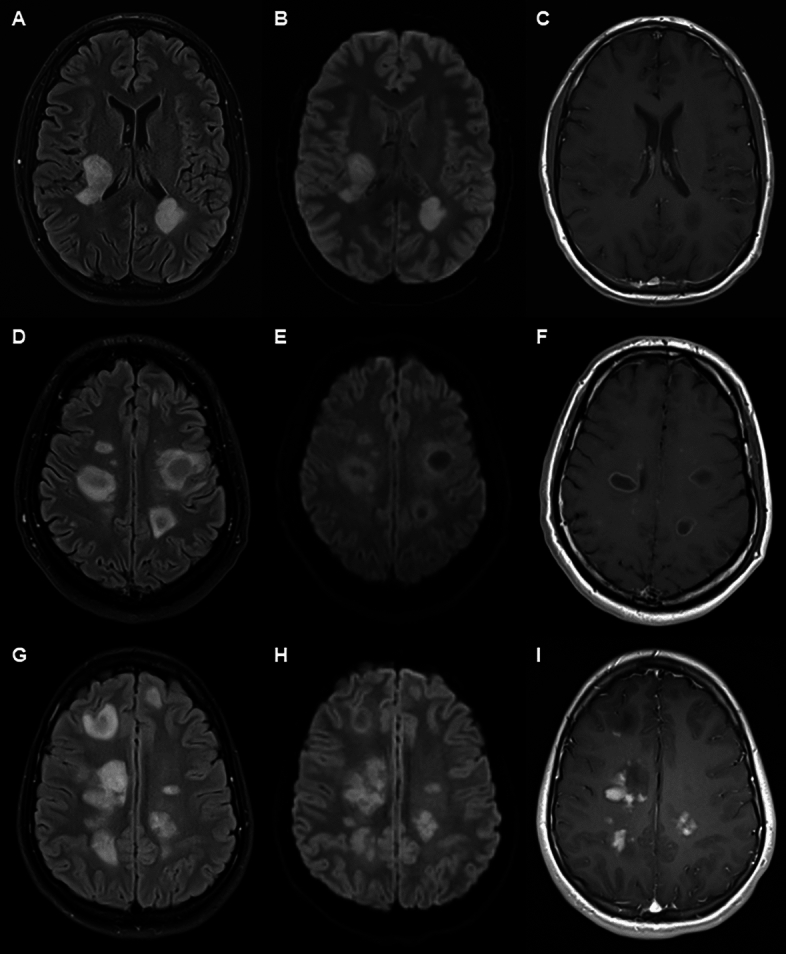
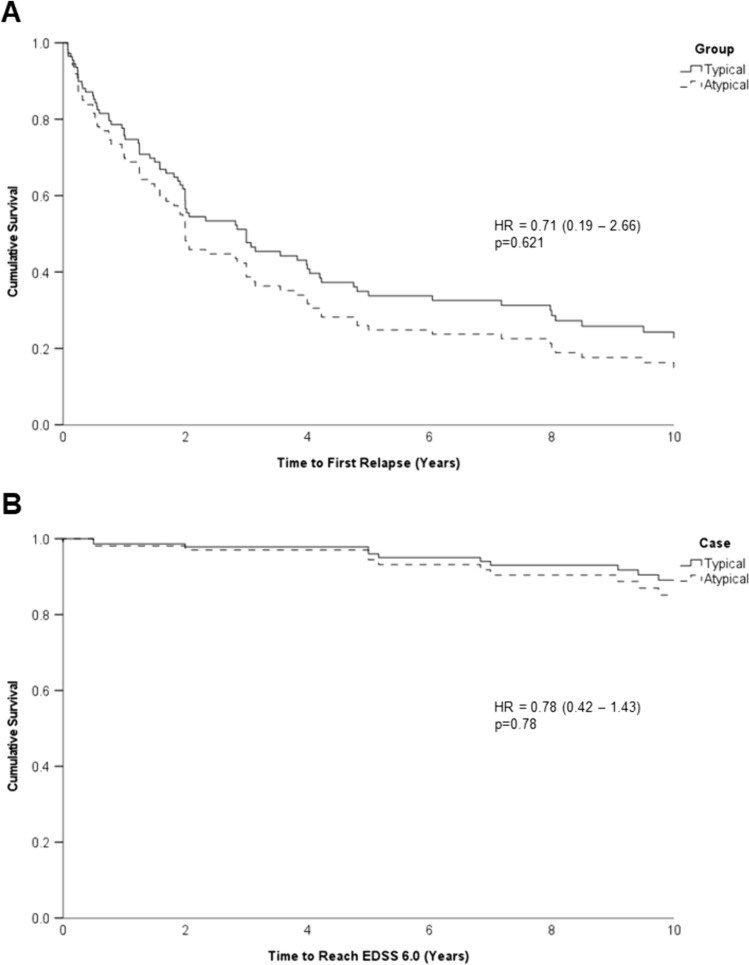
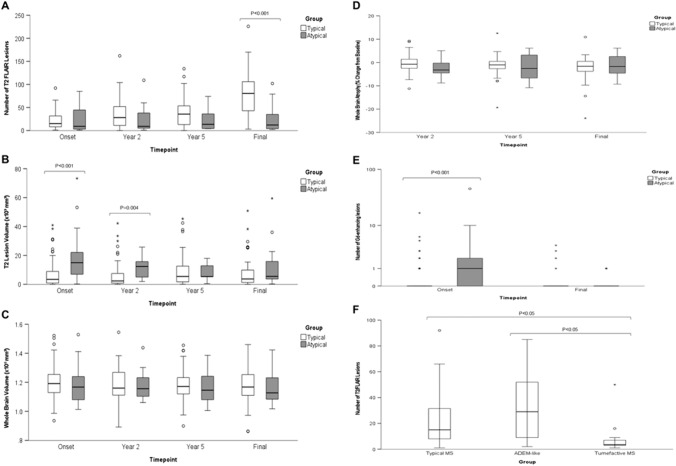
A minority of initial multiple sclerosis (MS) presentations clinically or radiologically resemble other central nervous system (CNS) pathologies, acute disseminated encephalomyelitis (ADEM) or tumefactive demyelination (atypical demyelination presentations). With the aim of better defining the long-term outcomes of this group we have performed a retrospective cohort comparison of atypical demyelination versus 'typical' MS presentations. Twenty-seven cases with atypical presentations (both first and subsequent demyelinating events) were identified and compared with typical MS cases. Disease features analysed included relapse rates, disability severity, whole brain and lesion volumes, lesion number and distribution. Atypical cases represented 3.9% of all MS cases. There was considerable overlap in the magnetic resonance imaging (MRI) features of ADEM-like and tumefactive demyelination cases. ADEM-like cases tended to be younger but not significantly so. Atypical cases showed a trend towards higher peak expanded disability severity score (EDSS) score at the time of their atypical presentation. Motor, cranial nerve, cerebellar, cerebral and multifocal presentations were all more common in atypical cases, and less likely to present with optic neuritis. Cerebrospinal fluid (CSF) white cell counts were higher in atypical cases (p = 0.002). One atypical case was associated with peripheral blood myelin oligodendrocyte glycoprotein (MOG) antibodies, but subsequent clinical and radiological course was in keeping with MS. There was no difference in long-term clinical outcomes including annualised relapse rates (ARR), brain volume, lesion numbers or lesion distributions. Atypical demyelination cases were more likely to receive high potency disease modifying therapy early in the course of their illness. Despite the severity of initial illness, our cohort analysis suggests that atypical demyelination presentations do not confer a higher risk of long-term adverse outcomes.
少数多发性硬化症 (MS) 的初始表现从临床或影像学上与其他中枢神经系统 (CNS) 病变相似,如急性播散性脑脊髓炎 (ADEM) 或肿块样脱髓鞘病变(非典型脱髓鞘表现)。为了更好地定义这组患者的长期结局,我们对非典型脱髓鞘与“典型”MS 表现进行了回顾性队列比较。我们确定了 27 例具有非典型表现(包括首次和随后的脱髓鞘事件)的病例,并与典型 MS 病例进行了比较。分析的疾病特征包括复发率、残疾严重程度、全脑和病变体积、病变数量和分布。非典型病例占所有 MS 病例的 3.9%。ADEM 样和肿块样脱髓鞘病变的 MRI 特征有很大的重叠。ADEM 样病例往往更年轻,但差异无统计学意义。非典型病例在非典型表现时的高峰扩展残疾严重程度评分 (EDSS) 较高,有一定的趋势。运动、颅神经、小脑、大脑和多灶性表现在非典型病例中更为常见,视神经炎的可能性较小。非典型病例的脑脊液 (CSF) 白细胞计数较高(p = 0.002)。1 例非典型病例与外周血髓鞘少突胶质细胞糖蛋白 (MOG) 抗体有关,但随后的临床和影像学病程符合 MS。长期临床结局无差异,包括年复发率 (ARR)、脑体积、病变数量或病变分布。非典型脱髓鞘病例更有可能在疾病早期接受高效疾病修正治疗。尽管初始疾病严重程度较高,但我们的队列分析表明,非典型脱髓鞘表现不会增加长期不良结局的风险。