Schottenfeld Richard S, Chawarski Marek C, Mazlan Mahmud
Department of Psychiatry, Yale University School of Medicine, New Haven, CT, USA.
Lancet. 2008 Jun 28;371(9631):2192-200. doi: 10.1016/S0140-6736(08)60954-X.
Expansion of access to effective treatments for heroin dependence is a worldwide health priority that will also reduce HIV transmission. We compared the efficacy of naltrexone, buprenorphine, and no additional treatment, in patients receiving detoxification and subsequent drug counselling, for maintenance of heroin abstinence, prevention of relapse, and reduction of HIV risk behaviours.
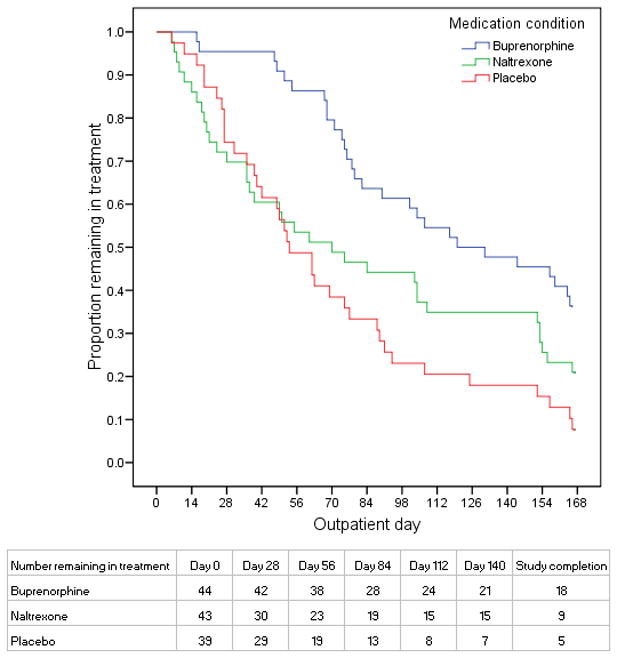
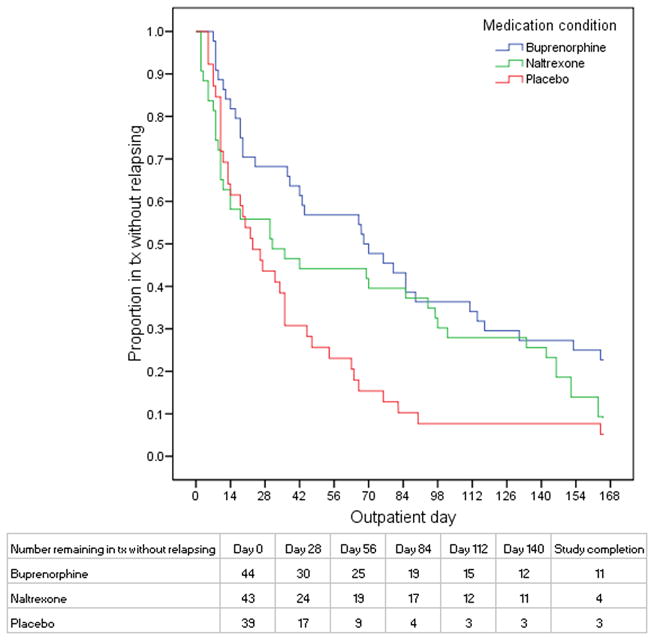
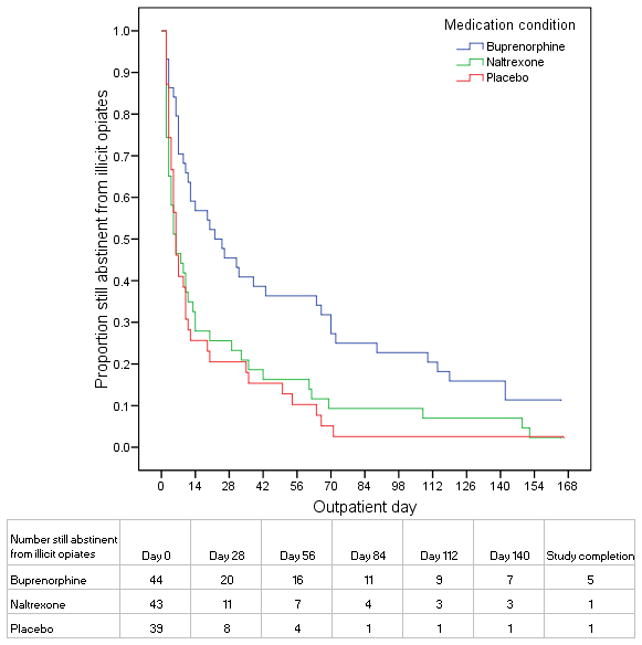
126 detoxified heroin-dependent patients, from an outpatient research clinic and detoxification programme in Malaysia, were randomly assigned by a computer-generated randomisation sequence to 24 weeks of manual-guided drug counselling and maintenance with naltrexone (n=43), buprenorphine (n=44), or placebo (n=39). Medications were administered on a double-blind and double-dummy basis. Primary outcomes, assessed by urine testing three times per week, were days to first heroin use, days to heroin relapse (three consecutive opioid-positive urine tests), maximum consecutive days of heroin abstinence, and reductions in HIV risk behaviours over 6 months. The study was terminated after 22 months of enrolment because buprenorphine was shown to have greater efficacy in an interim safety analysis. Analysis was by intention to treat. This study is registered with ClinicalTrials.gov, number NCT00383045.
We observed consistent, linear contrasts in days to first heroin use (p=0.0009), days to heroin relapse (p=0.009), and maximum consecutive days abstinent (p=0.0007), with all results best for buprenorphine and worst for placebo. Buprenorphine was associated with greater time to first heroin use than were naltrexone (hazard ratio 1.87 [95% CI 1.21-2.88]) or placebo (2.02 [1.29-3.16]). With buprenorphine, we also recorded significantly greater time to heroin relapse (2.17 [1.38-3.42]), and maximum consecutive days abstinent than with placebo (mean days 59 [95% CI 43-76] vs 24 [13-35]; p=0.003); however, for these outcomes, differences between buprenorphine and naltrexone were not significant. Differences between naltrexone and placebo were not significant for any outcomes. HIV risk behaviours were significantly reduced from baseline across all three treatments (p=0.003), but the reductions did not differ significantly between the three groups.
Our findings lend support to the widespread dissemination of maintenance treatment with buprenorphine as an effective public-health approach to reduce problems associated with heroin dependence.
扩大获得有效治疗海洛因依赖的途径是一项全球卫生重点工作,这也将减少艾滋病毒传播。我们比较了纳曲酮、丁丙诺啡以及不进行额外治疗,在接受戒毒及后续药物咨询的患者中,维持海洛因戒断、预防复发以及减少艾滋病毒风险行为方面的疗效。
来自马来西亚一家门诊研究诊所和戒毒项目的126名已戒毒的海洛因依赖患者,通过计算机生成的随机序列被随机分配至接受为期24周的手工指导药物咨询,并分别使用纳曲酮维持治疗(n = 43)、丁丙诺啡维持治疗(n = 44)或安慰剂维持治疗(n = 39)。药物采用双盲双模拟方式给药。主要结局指标通过每周三次尿液检测进行评估,包括首次使用海洛因的天数、海洛因复发天数(连续三次阿片类药物阳性尿液检测)、海洛因戒断的最长连续天数以及6个月内艾滋病毒风险行为的减少情况。在入组22个月后,该研究终止,因为在一项中期安全性分析中显示丁丙诺啡具有更高的疗效。分析采用意向性分析。本研究已在ClinicalTrials.gov注册,编号为NCT00383045。
我们观察到在首次使用海洛因的天数(p = 0.0009)、海洛因复发天数(p = 0.009)和最长连续戒断天数(p = 0.0007)方面存在一致的线性差异,所有结果均显示丁丙诺啡最佳,安慰剂最差。丁丙诺啡组相比纳曲酮组(风险比1.87 [95%可信区间1.21 - 2.88])或安慰剂组(2.02 [1.29 - 3.16]),首次使用海洛因的时间更长。使用丁丙诺啡时,我们还记录到相比安慰剂组,海洛因复发的时间显著更长(2.17 [1.38 - 3.42]),以及最长连续戒断天数更多(平均天数59 [95%可信区间43 - 76] 对24 [13 - 35];p = 0.003);然而,对于这些结局指标,丁丙诺啡与纳曲酮之间的差异并不显著。纳曲酮与安慰剂在任何结局指标上的差异均不显著。在所有三种治疗中,艾滋病毒风险行为均较基线显著减少(p = 0.003),但三组之间的减少幅度没有显著差异。
我们的研究结果支持广泛推广丁丙诺啡维持治疗,将其作为一种有效的公共卫生方法,以减少与海洛因依赖相关的问题。