Wu Bechien U, Johannes Richard S, Kurtz Stephen, Banks Peter A
Division of Gastroenterology, Brigham and Women's Hospital, Center for Pancreatic Disease, Harvard Medical School, Boston, Massachusetts 02115, USA.
Gastroenterology. 2008 Sep;135(3):816-20. doi: 10.1053/j.gastro.2008.05.053. Epub 2008 May 28.
BACKGROUND & AIMS: Little is known regarding the impact of hospital-acquired infection (HAI) in acute pancreatitis (AP). We conducted a population-based assessment of the impact of HAI on outcome in AP.
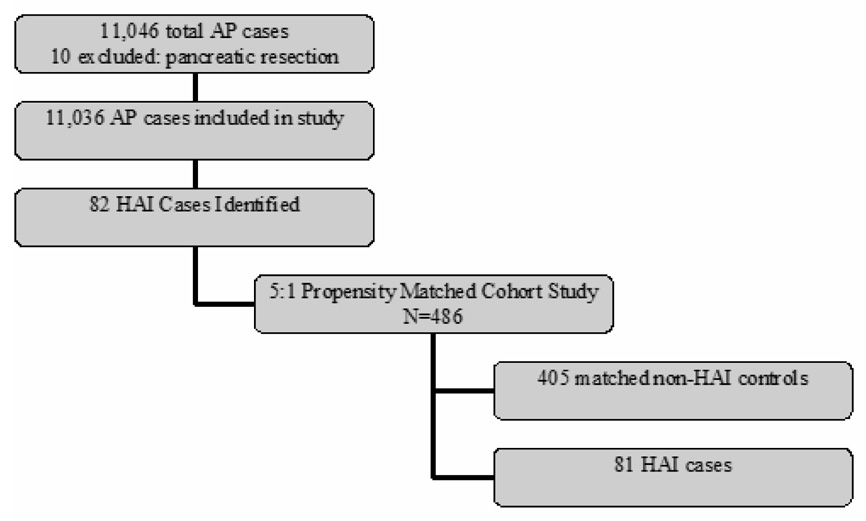
Patient data were obtained from the Cardinal Health Clinical Outcomes Research Database, a large population-based data set. Cases with principal diagnosis by International Classification of Diseases, ninth revision, clinical modification 577.0 (AP) between January 2004 and January 2005 were identified. These cases were linked with recently reported HAI data collected by the Pennsylvania Health Care Cost Containment Council. Identification of HAI was based on definitions set forth by the National Nosocomial Infection Surveillance System. We conducted a 5:1 multivariate propensity-matched cohort study to determine the independent contribution of HAI to in-hospital mortality, length of stay (LOS), and hospital charges.
From 177 participating hospitals, there were 11,046 AP cases identified. Eighty-two (0.7%) patients developed an HAI. Mortality in the overall AP population was 1.2% vs 11.4% among 405 matched non-HAI controls vs 28.4% among patients who developed HAI (chi(2) test, P < .0001). Fifteen percent of all deaths was associated with an HAI. Both average LOS and hospital charges were significantly increased among patients with HAI compared with matched non-HAI controls.
We determined that HAI had a major impact on mortality in AP. Patients who developed HAI also had significantly increased LOS and hospital charges. These differences were not explained by increased disease severity alone. Reducing HAI is an important step to improving outcome in AP.
关于医院获得性感染(HAI)对急性胰腺炎(AP)的影响,目前所知甚少。我们基于人群评估了HAI对AP预后的影响。
患者数据来自红衣主教健康临床结局研究数据库,这是一个基于大量人群的数据集。确定2004年1月至2005年1月期间国际疾病分类第九版临床修订本577.0(AP)主要诊断的病例。这些病例与宾夕法尼亚医疗成本控制委员会最近报告的HAI数据相关联。HAI的识别基于国家医院感染监测系统规定的定义。我们进行了一项5:1的多变量倾向匹配队列研究,以确定HAI对住院死亡率、住院时间(LOS)和医院费用的独立影响。
从177家参与医院中,共识别出11046例AP病例。82例(0.7%)患者发生了HAI。总体AP人群的死亡率为1.2%,405例匹配的非HAI对照组为11.4%,发生HAI的患者为28.4%(卡方检验,P <.0001)。所有死亡病例中有15%与HAI相关。与匹配的非HAI对照组相比,发生HAI的患者平均LOS和医院费用均显著增加。
我们确定HAI对AP的死亡率有重大影响。发生HAI的患者LOS和医院费用也显著增加。这些差异不能仅用疾病严重程度增加来解释。减少HAI是改善AP预后的重要一步。