Mubyazi Godfrey M, Bygbjerg Ib C, Magnussen Pascal, Olsen Oystein, Byskov Jens, Hansen Kristian S, Bloch Paul
National Institute for Medical Research, Dar-es-Salaam, Tanzania.
Malar J. 2008 Jul 22;7:135. doi: 10.1186/1475-2875-7-135.
To describe the prospects, achievements, challenges and opportunities for implementing intermittent preventive treatment for malaria in pregnancy (IPTp) in Tanzania in light of national antenatal care (ANC) guidelines and ability of service providers to comply with them.
In-depth interviews were made with national level malaria control officers in 2006 and 2007. Data was analysed manually using a qualitative content analysis approach.
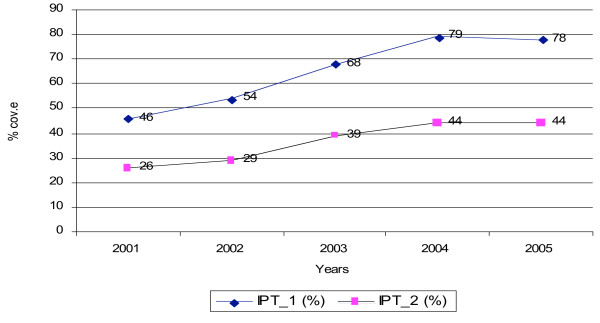
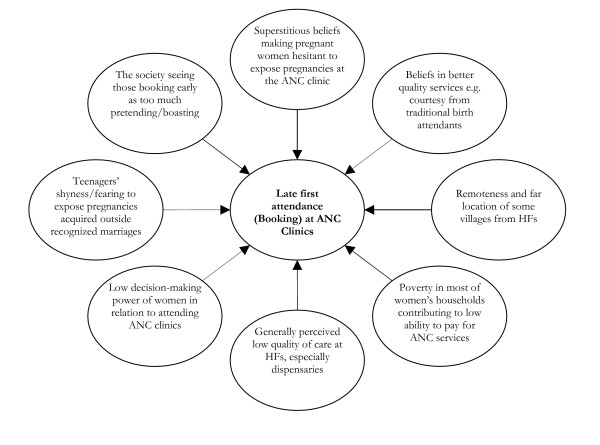
IPTp has been under implementation countrywide since 2001 and the 2005 evaluation report showed increased coverage of women taking two doses of IPTp from 29% to 65% between 2001 and 2007. This achievement was acknowledged, however, several challenges were noted including (i) the national antenatal care (ANC) guidelines emphasizing two IPTp doses during a woman's pregnancy, while other agencies operating at district level were recommending three doses, this confuses frontline health workers (HWs); (ii) focused ANC guidelines have been revised, but printing and distribution to districts has often been delayed; (iii) reports from district management teams demonstrate constraints related to women's late booking, understaffing, inadequate skills of most HWs and their poor motivation. Other problems were unreliable supply of free SP at private clinics, clean and safe water shortage at many government ANC clinics limiting direct observation treatment and occasionally pregnant women asked to pay for ANC services. Finally, supervision of peripheral health facilities has been inadequate and national guidelines on district budgeting for health services have been inflexible. IPTp coverage is generally low partly because IPTp is not systematically enforced like programmes on immunization, tuberculosis, leprosy and other infectious diseases. Necessary concerted efforts towards fostering uptake and coverage of two IPTp doses were emphasized by the national level officers, who called for further action including operational health systems research to understand challenges and suggest ways forward for effective implementation and high coverage of IPTp.
The benefit of IPTp is appreciated by national level officers who are encouraged by trends in the coverage of IPTp doses. However, their appeal for concerted efforts towards IPTp scaling-up through rectifying the systemic constraints and operational research is important and supported by suggestions by other authors.
根据坦桑尼亚国家产前保健(ANC)指南以及服务提供者遵守这些指南的能力,描述在坦桑尼亚实施孕期疟疾间歇性预防治疗(IPTp)的前景、成就、挑战和机遇。
在2006年和2007年对国家级疟疾控制官员进行了深入访谈。使用定性内容分析方法对数据进行人工分析。
自2001年以来,IPTp已在全国范围内实施,2005年的评估报告显示,在2001年至2007年期间,接受两剂IPTp的妇女覆盖率从29%提高到了65%。这一成就得到了认可,然而,也指出了一些挑战,包括:(i)国家产前保健(ANC)指南强调在妇女怀孕期间给予两剂IPTp,而在地区层面运作的其他机构则建议给予三剂,这使一线卫生工作者(HWs)感到困惑;(ii)重点突出的ANC指南已经修订,但向各地区的印刷和分发工作经常延迟;(iii)地区管理团队的报告表明存在与妇女预约过晚、人员配备不足、大多数HWs技能不足及其积极性不高相关的制约因素。其他问题包括私立诊所免费磺胺多辛-乙胺嘧啶(SP)供应不可靠、许多政府ANC诊所清洁安全用水短缺限制了直接观察治疗,以及偶尔有孕妇被要求支付ANC服务费用。最后,对基层卫生设施的监督不足,而且关于地区卫生服务预算的国家指南缺乏灵活性。IPTp覆盖率总体较低,部分原因是IPTp不像免疫、结核病、麻风病和其他传染病项目那样得到系统执行。国家级官员强调了为提高两剂IPTp的接受率和覆盖率而做出必要协同努力的重要性,他们呼吁采取进一步行动,包括开展业务卫生系统研究,以了解挑战并提出有效实施IPTp和提高其覆盖率的前进方向。
国家级官员认识到IPTp的益处,IPTp剂量覆盖率的趋势也鼓舞了他们。然而,他们呼吁通过纠正系统性制约因素和开展业务研究来协同努力扩大IPTp规模,这一点很重要,并且得到了其他作者建议的支持。