Parienti Jean-Jacques, Das-Douglas Moupali, Massari Véronique, Guzman David, Deeks Steven G, Verdon Renaud, Bangsberg David R
Clinical Research and Biostatistics Department, Côte de Nacre University Hospital, Caen, France.
PLoS One. 2008 Jul 30;3(7):e2783. doi: 10.1371/journal.pone.0002783.
While the relationship between average adherence to HIV potent antiretroviral therapy is well defined, the relationship between patterns of adherence within adherence strata has not been investigated. We examined medication event monitoring system (MEMS) defined adherence patterns and their relation to subsequent virologic rebound.
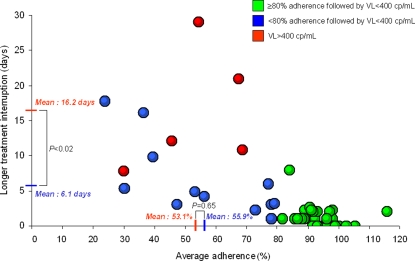
We selected subjects with at least 3-months of previous virologic suppression on a non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimen from two prospective cohorts in France and North America. We assessed the risk of virologic rebound, defined as HIV RNA of >400 copies/mL according to several MEMS adherence measurements. Seventy two subjects were studied, five of them experienced virologic rebound. Subjects with and without virologic rebound had similar baseline characteristics including treatment durations, regimen (efavirenz vs nevirapine), and dosing schedule. Each 10% increase in average adherence decreased the risk of virologic rebound (OR = 0.56; 95% confidence interval (CI) [0.37, 0.81], P<0.002). Each additional consecutive day off therapy for the longest treatment interruption (OR = 1.34; 95%CI [1.15, 1.68], P<0.0001) and each additional treatment interruption for more than 2 days (OR = 1.38; 95%CI [1.13, 1.77], P<0.002) increased the risk of virologic rebound. In those with low-to-moderate adherence (i.e. <80%), treatment interruption duration (16.2 days versus 6.1 days in the control group, P<0.02), but not average adherence (53.1% vs 55.9%, respectively, P = 0.65) was significantly associated with virologic rebound.
Sustained treatment interruption may pose a greater risk of virologic rebound on NNRTI therapy than the same number of interspersed missed doses at low-to-moderate adherence.
虽然高效抗逆转录病毒疗法的平均依从性与疗效之间的关系已明确,但依从性分层内的依从模式之间的关系尚未得到研究。我们研究了药物事件监测系统(MEMS)定义的依从模式及其与随后病毒学反弹的关系。
我们从法国和北美的两个前瞻性队列中选取了此前至少3个月采用基于非核苷类逆转录酶抑制剂(NNRTI)方案实现病毒学抑制的受试者。根据多种MEMS依从性测量指标,我们评估了病毒学反弹的风险,病毒学反弹定义为HIV RNA>400拷贝/mL。共研究了72名受试者,其中5人出现病毒学反弹。出现和未出现病毒学反弹的受试者具有相似的基线特征,包括治疗持续时间、治疗方案(依非韦伦与奈韦拉平)和给药方案。平均依从性每提高10%,病毒学反弹风险降低(比值比[OR]=0.56;95%置信区间[CI][0.37, 0.81],P<0.002)。最长治疗中断每增加连续停药1天(OR = 1.34;95%CI[1.15, 1.68],P<0.0001)以及每增加一次超过2天的治疗中断(OR = 1.38;95%CI[1.13, 1.77],P<0.002),病毒学反弹风险增加。在依从性低至中等(即<80%)的受试者中,治疗中断持续时间(16.2天对比对照组的6.1天,P<0.02)而非平均依从性(分别为53.1%对比55.9%,P = 0.65)与病毒学反弹显著相关。
在低至中等依从性情况下,持续的治疗中断可能比相同次数的分散漏服剂量在NNRTI治疗中带来更高的病毒学反弹风险。