Winickoff Jonathan P, Park Elyse R, Hipple Bethany J, Berkowitz Anna, Vieira Cecilia, Friebely Joan, Healey Erica A, Rigotti Nancy A
Center for Child and Adolescent Health Policy, 50 Staniford St, Suite 901, Boston, MA 02114, USA.
Pediatrics. 2008 Aug;122(2):e363-75. doi: 10.1542/peds.2008-0478.
The purpose of this work was to describe a novel process and present results of formative research to develop a pediatric office intervention that uses available systems of care for addressing parental smoking.
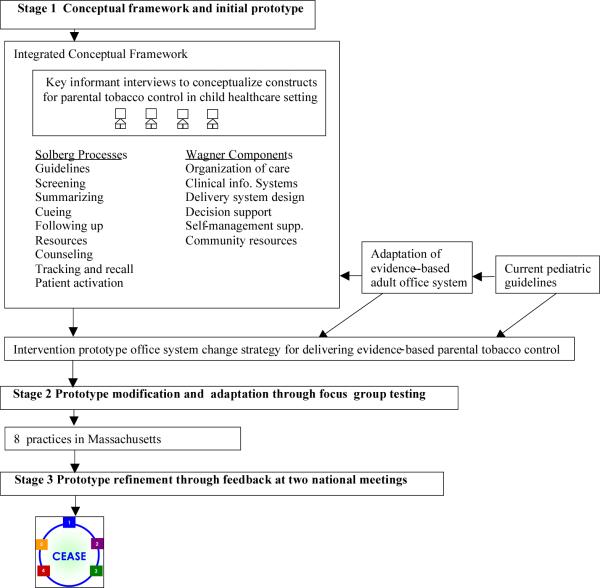
The scientific development of the intervention occurred in 3 stages. In stage 1, we designed an office system for parental tobacco control in the pediatric outpatient setting on the basis of complementary conceptual frameworks of preventive services delivery, conceptualized for the child health care setting through a process of key interviews with leaders in the field of implementing practice change; existing Public Health Service guidelines that had been shown effective in adult practices; and adaptation of an evidence-based adult office system for tobacco control. This was an iterative process that yielded a theoretically framed intervention prototype. In stage 2, we performed focus-group testing in pediatric practices with pediatricians, nurses, clinical assistants, and key office staff. Using qualitative methods, we adapted the intervention prototype on the basis of this feedback to include 5 key implementation steps for the child health care setting. In stage 3, we presented the intervention to breakout groups at 2 national meetings of pediatric practitioners for additional refinements.
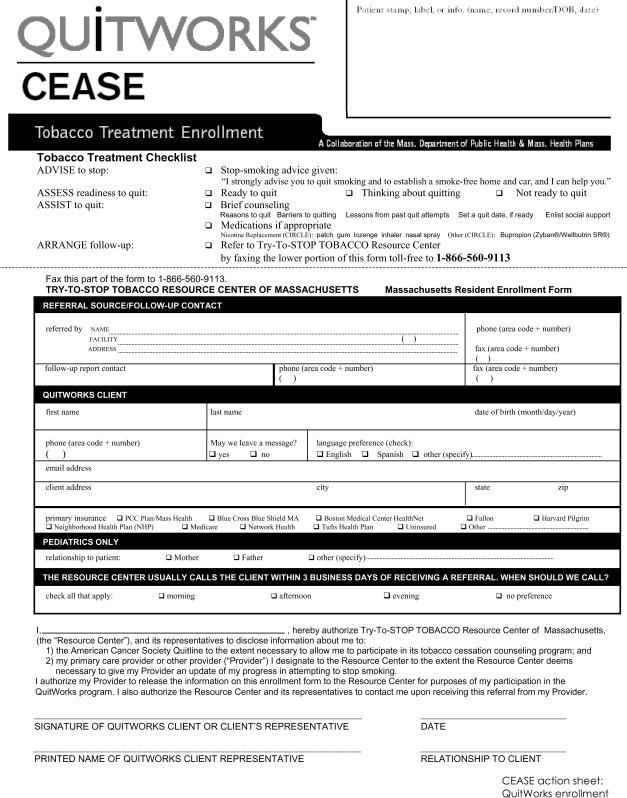
The main result was a theoretically grounded intervention that was responsive to the barriers and suggestions raised in the focus groups and at the national meetings. The Clinical Effort Against Secondhand Smoke Exposure intervention was designed to be flexible and adaptable to the particular practices' staffing, resources, and physical configuration. Practice staff can choose materials relevant to their own particular systems of care (www.ceasetobacco.org).
Conceptually grounded and focus-group-tested strategies for parental tobacco control are now available for implementation in the pediatric outpatient setting. The tobacco-control intervention-development process might have particular relevance for other chronic pediatric conditions that have a strong evidence base and have available treatments or resources that are underused.
本研究旨在描述一种新方法,并展示形成性研究的结果,以开发一种儿科门诊干预措施,利用现有的医疗体系来解决家长吸烟问题。
该干预措施的科学开发分三个阶段进行。在第一阶段,我们基于预防性服务提供的互补概念框架,设计了一个儿科门诊环境中家长烟草控制的办公系统。通过与实施实践变革领域的领导者进行关键访谈,为儿童保健环境进行概念化;已证明在成人实践中有效的现有公共卫生服务指南;以及对基于证据的成人烟草控制办公系统的改编。这是一个迭代过程,产生了一个理论框架下的干预原型。在第二阶段,我们在儿科诊所对儿科医生、护士、临床助理和关键办公人员进行了焦点小组测试。使用定性方法,我们根据反馈对干预原型进行了调整,以纳入儿童保健环境的5个关键实施步骤。在第三阶段,我们在两次全国儿科从业者会议上向分组讨论小组介绍了该干预措施,以进行进一步完善。
主要结果是一种基于理论的干预措施,对焦点小组和全国会议上提出的障碍和建议做出了回应。“临床防治二手烟暴露”干预措施旨在具有灵活性,能够适应特定诊所的人员配备、资源和物理配置。诊所工作人员可以选择与其自身特定医疗体系相关的材料(www.ceasetobacco.org)。
现在有了基于概念且经过焦点小组测试的家长烟草控制策略,可在儿科门诊环境中实施。烟草控制干预措施的开发过程可能与其他有充分证据基础且有可用但未充分利用的治疗方法或资源的儿童慢性疾病特别相关。