Hoff M, Kvien T K, Kälvesten J, Elden A, Haugeberg G
Department of Rheumatology, St Olav's Hospital, Trondheim, Norway.
Ann Rheum Dis. 2009 Jul;68(7):1171-6. doi: 10.1136/ard.2008.091264. Epub 2008 Sep 18.
The effect of adalimumab on hand osteoporosis was examined and related to radiographic joint damage in the three treatment arms of the PREMIER study: adalimumab plus methotrexate, adalimumab and methotrexate monotherapy. Predictors of hand bone loss were also searched for.
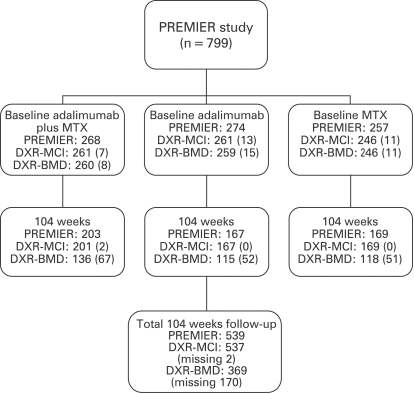
768 patients (537 fulfilled 2 years) with rheumatoid arthritis (RA) for less than 3 years, never treated with methotrexate, were included. Hand bone loss was assessed by digital x ray radiogrammetry (DXR) on the same hand radiographs scored with modified Sharp score at baseline, 26, 52 and 104 weeks. For DXR, metacarpal cortical index (MCI) was the primary bone measure.
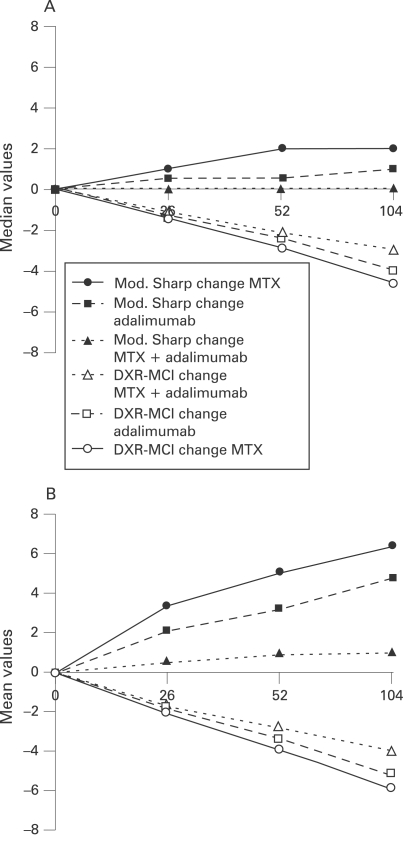
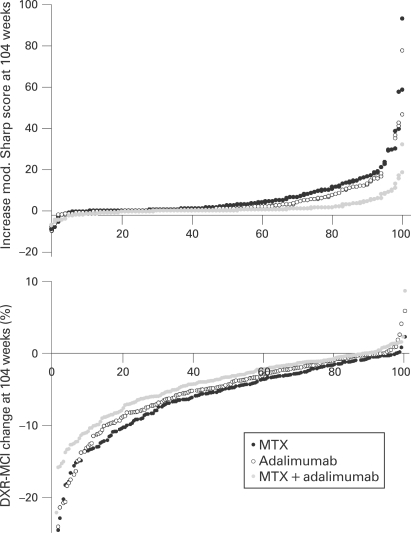
At all time points the rate of percentage DXR-MCI loss was lowest in the combination group (-1.15; -2.16; -3.03) and greatest in the methotrexate monotherapy group (-1.42; -2.87; -4.62), with figures in between for the adalimumab monotherapy group (-1.33; -2.45; -4.03). Significant differences between the combination group and the methotrexate group were seen at 52 (p = 0.009) and 104 weeks (p<0.001). The order of hand bone loss across the three treatment arms was similar to the order of radiographic progression. Older age, elevated C-reactive protein and non-use of adalimumab were predictors of hand bone loss.
This study supports a similar pathogenic mechanism for hand bone loss and erosions in RA. The combination of adalimumab and methotrexate seems to arrest hand bone loss less effectively than radiographic joint damage. Quantitative measures of osteoporosis may thus be a more sensitive tool for assessment of inflammatory bone involvement in RA.
在PREMIER研究的三个治疗组中,即阿达木单抗联合甲氨蝶呤组、阿达木单抗组和甲氨蝶呤单药治疗组,研究阿达木单抗对手部骨质疏松的影响,并将其与影像学关节损伤相关联。同时还探寻了手部骨质流失的预测因素。
纳入768例类风湿关节炎(RA)病程小于3年且从未接受过甲氨蝶呤治疗的患者(537例完成了2年的研究)。通过数字X线放射计量法(DXR)在基线、26周、52周和104周时对同一手部X线片进行手部骨质流失评估,这些X线片同时用改良Sharp评分法进行评分。对于DXR,掌骨皮质指数(MCI)是主要的骨测量指标。
在所有时间点,联合治疗组的DXR-MCI丢失率百分比最低(-1.15;-2.16;-3.03),甲氨蝶呤单药治疗组最高(-1.42;-2.87;-4.62),阿达木单抗单药治疗组介于两者之间(-1.33;-2.45;-4.03)。联合治疗组与甲氨蝶呤组在52周(p = 0.009)和104周(p<0.001)时存在显著差异。三个治疗组的手部骨质流失顺序与影像学进展顺序相似。年龄较大、C反应蛋白升高以及未使用阿达木单抗是手部骨质流失的预测因素。
本研究支持RA中手部骨质流失和侵蚀具有相似的致病机制。阿达木单抗与甲氨蝶呤联合使用似乎在阻止手部骨质流失方面不如阻止影像学关节损伤有效。因此,骨质疏松的定量测量可能是评估RA中炎症性骨受累的更敏感工具。