Tam Lily W Y, Chui Celia K S, Brumme Chanson J, Bangsberg David R, Montaner Julio S G, Hogg Robert S, Harrigan P Richard
British Columbia Centre for Excellence in HIV/AIDS, Vancouver, British Columbia, Vancouver, Canada.
J Acquir Immune Defic Syndr. 2008 Nov 1;49(3):266-71. doi: 10.1097/QAI.0b013e318189a753.
To investigate the relationship between HIV-1 drug resistance and adherence and the accumulation rate of resistance mutations in 1191 HIV-infected, antiretroviral-naive adults initiating highly active antiretroviral therapy in British Columbia, Canada.
Plasma samples with plasma viral load >1,000 copies per milliliter collected within 30 months of follow-up were genotyped for drug resistance. Adherence was estimated using prescription refills and plasma drug levels. The primary outcome measure was time to detection of drug resistance. Cox proportional hazard regression was used to calculate hazard ratios (HRs) associated with baseline variables.
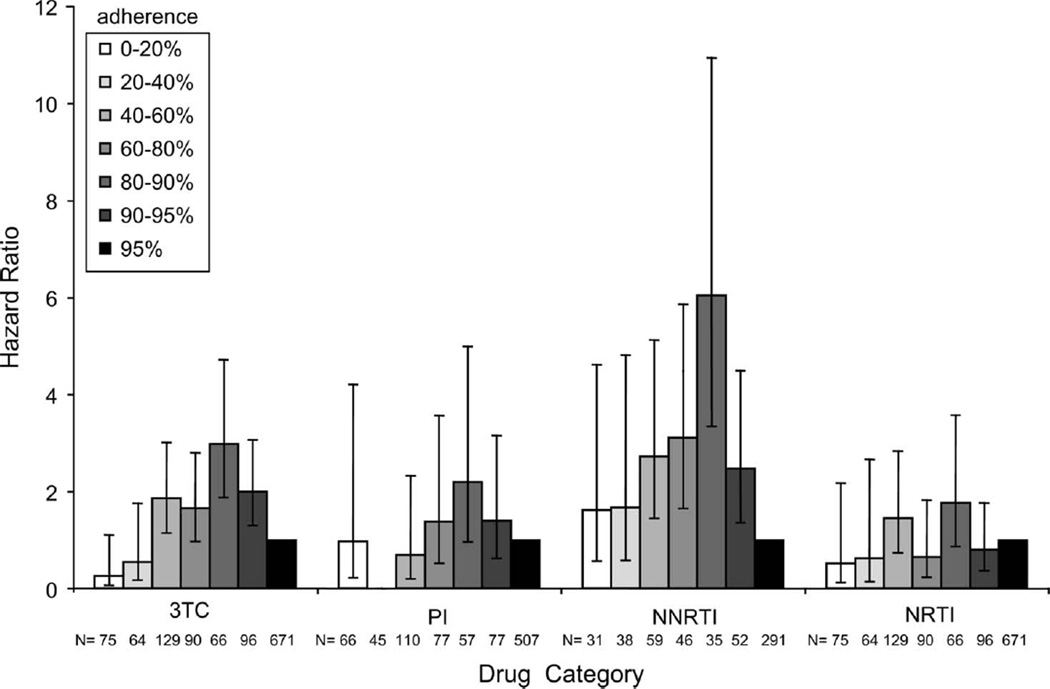
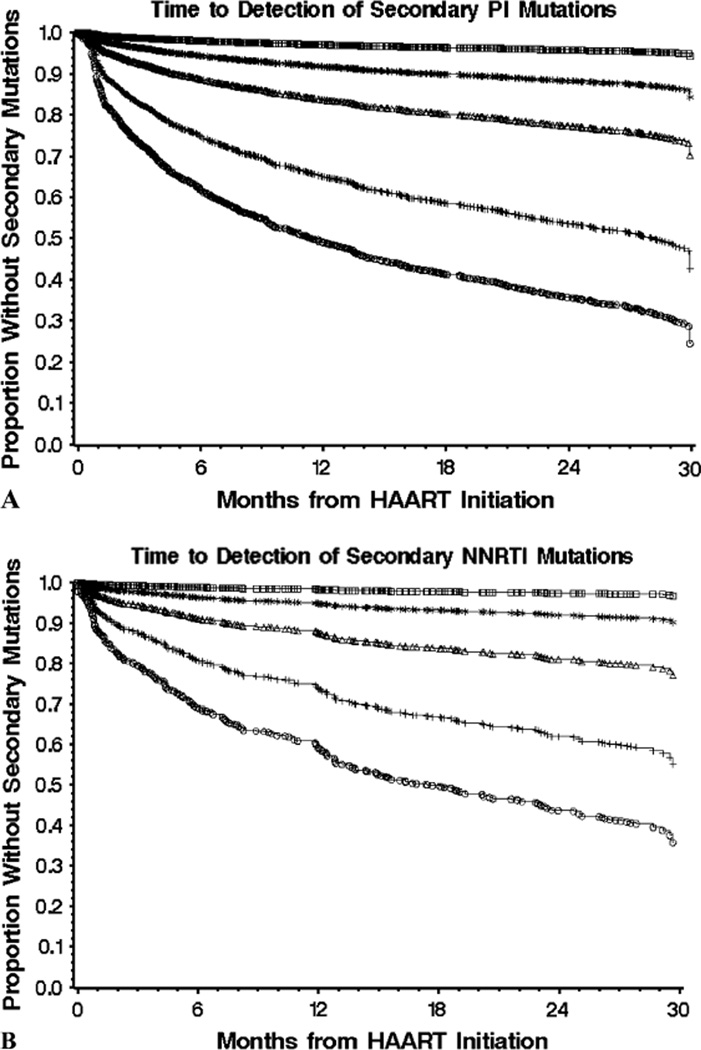
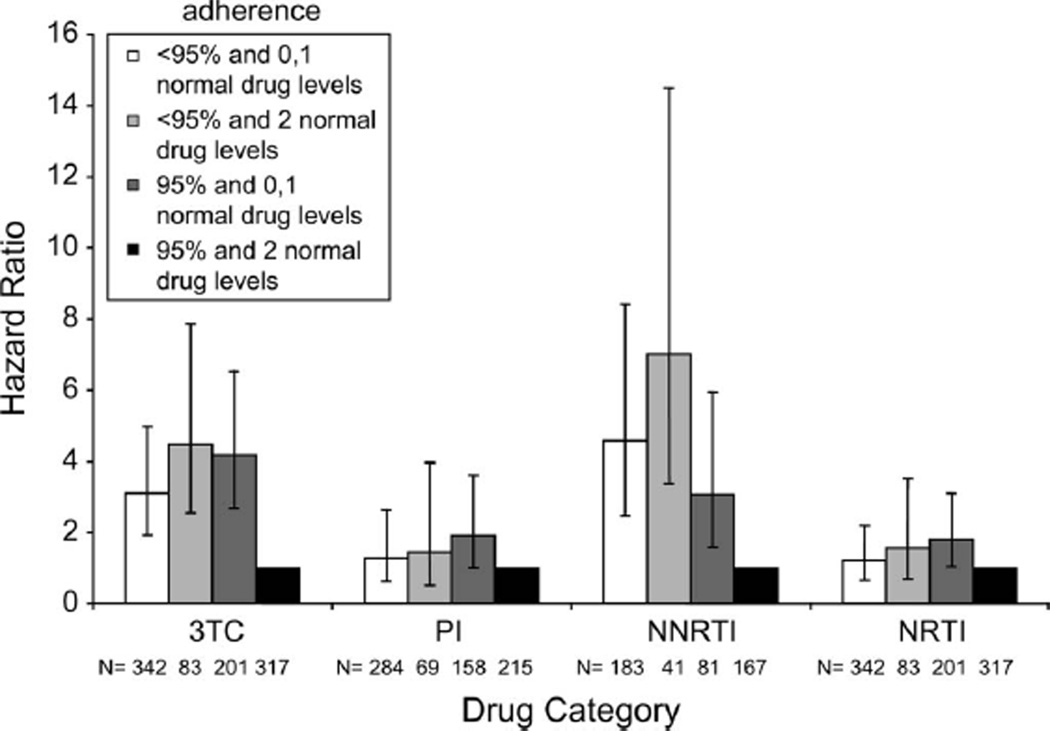
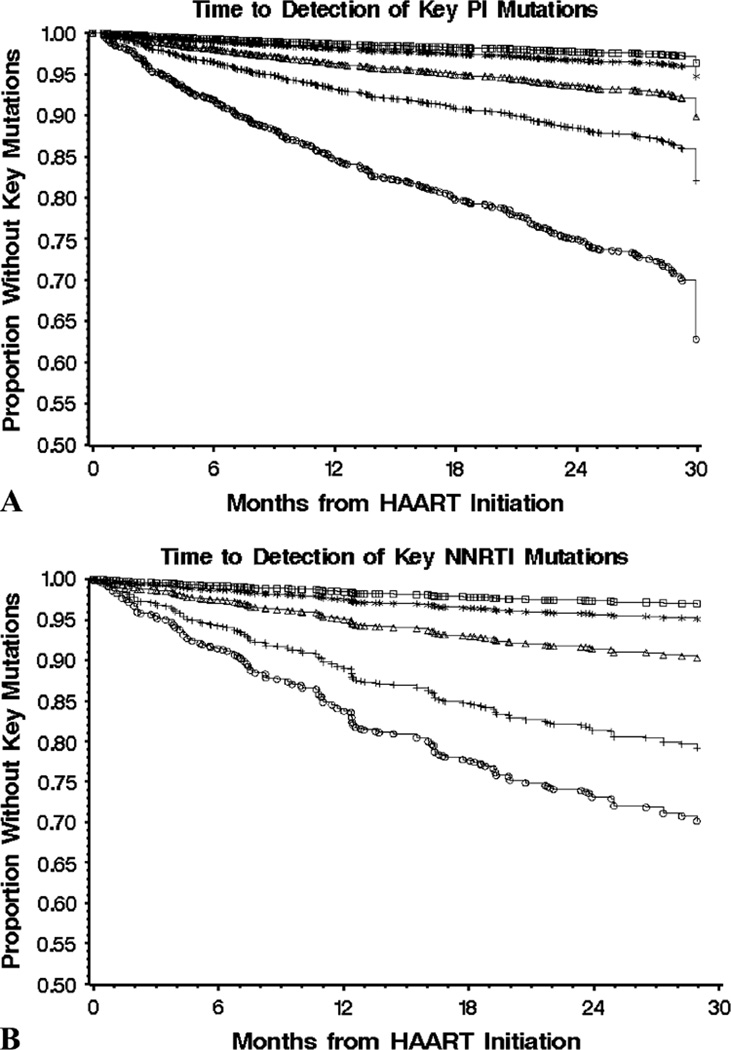
The accumulation rates of multiple primary and secondary mutations were similar in patients initiating highly active antiretroviral therapy with protease inhibitor versus nonnucleoside reverse transcriptase inhibitor (NNRTI). Rates decreased approximately 50% per additional mutation. At 80%-90% adherence based on refills, there was greater risk of detecting lamivudine (3TC) [HR 3.0, 95% confidence interval (CI): 1.9 to 4.7; P < 0.0001] and NNRTI mutations (HR 6.0, 95% CI: 3.3 to 10.9; P < 0.0001) compared with the >or=95% refill reference group. In a multivariate model, individuals with <95% refills and consistently detectable plasma drug levels were at increased risk for 3TC (HR 4.5, 95% CI: 2.6 to 7.9; P = 0.0001) and NNRTI resistance (HR 7.0, 95% CI: 3.4 to 14.5; P = 0.0001) compared with the reference group of >or=95% refills with consistently detectable drug levels. Adherence-resistance relationships were much weaker for protease inhibitors and nucleoside reverse transcriptase inhibitors as there was little variance in HRs among the different adherence strata compared with 3TC and NNRTIs.
The relationships between resistance, adherence, and mutation accumulation differ between HIV drug classes.
在加拿大不列颠哥伦比亚省1191名开始接受高效抗逆转录病毒治疗的初治成人HIV感染者中,研究HIV - 1耐药性与依从性以及耐药突变积累率之间的关系。
对随访30个月内收集的血浆病毒载量>1000拷贝/毫升的血浆样本进行耐药基因分型。使用处方 refill 和血浆药物水平评估依从性。主要结局指标是检测到耐药性的时间。采用Cox比例风险回归计算与基线变量相关的风险比(HRs)。
开始使用蛋白酶抑制剂与非核苷类逆转录酶抑制剂(NNRTI)进行高效抗逆转录病毒治疗的患者中,多种主要和次要突变的积累率相似。每增加一个突变,积累率下降约50%。基于refill,依从性在80% - 90%时,与≥95% refill参考组相比,检测到拉米夫定(3TC)耐药的风险更高[HR 3.0,95%置信区间(CI):1.9至4.7;P < 0.0001],检测到NNRTI突变的风险更高(HR 6.0,95% CI:3.3至10.9;P < 0.0001)。在多变量模型中,与refill≥95%且血浆药物水平持续可检测的参考组相比,refill<95%且血浆药物水平持续可检测的个体发生3TC耐药(HR 4.5,95% CI:2.6至7.9;P = 0.0001)和NNRTI耐药(HR 7.0,95% CI:3.4至14.5;P = 0.0001)的风险增加。与3TC和NNRTIs相比,蛋白酶抑制剂和核苷类逆转录酶抑制剂的依从性 - 耐药性关系要弱得多,因为不同依从性分层之间的HRs差异很小。
HIV药物类别之间,耐药性、依从性和突变积累之间的关系有所不同。