Pongtavornpinyo Wirichada, Yeung Shunmay, Hastings Ian M, Dondorp Arjen M, Day Nicholas P J, White Nicholas J
Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Malar J. 2008 Nov 2;7:229. doi: 10.1186/1475-2875-7-229.
Most malaria-endemic countries are implementing a change in anti-malarial drug policy to artemisinin-based combination therapy (ACT). The impact of different drug choices and implementation strategies is uncertain. Data from many epidemiological studies in different levels of malaria endemicity and in areas with the highest prevalence of drug resistance like borders of Thailand are certainly valuable. Formulating an appropriate dynamic data-driven model is a powerful predictive tool for exploring the impact of these strategies quantitatively.
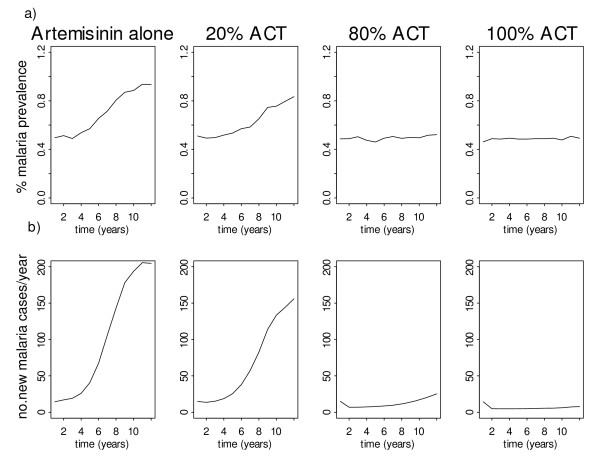
A comprehensive model was constructed incorporating important epidemiological and biological factors of human, mosquito, parasite and treatment. The iterative process of developing the model, identifying data needed, and parameterization has been taken to strongly link the model to the empirical evidence. The model provides quantitative measures of outcomes, such as malaria prevalence/incidence and treatment failure, and illustrates the spread of resistance in low and high transmission settings. The model was used to evaluate different anti-malarial policy options focusing on ACT deployment.
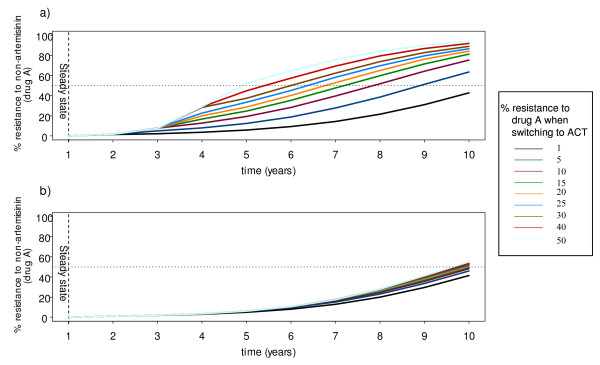
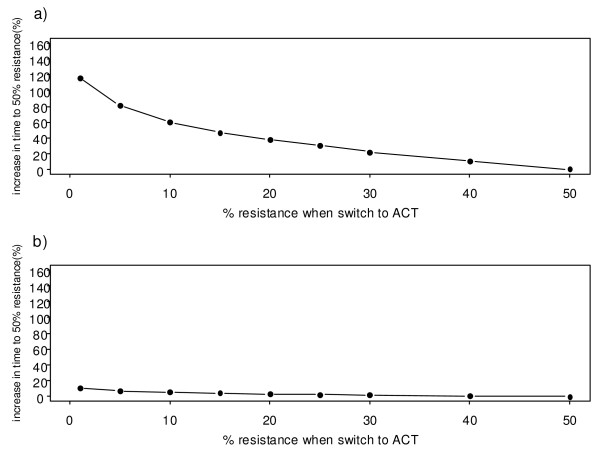
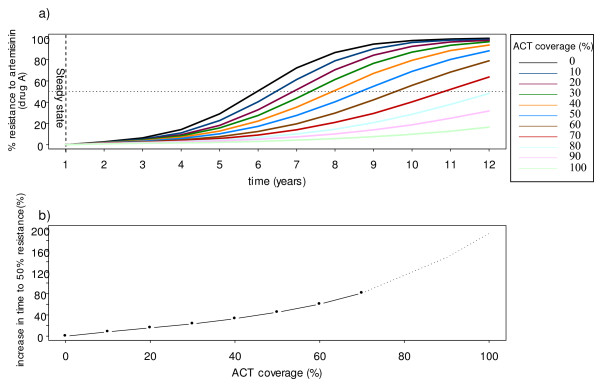
The model predicts robustly that in low transmission settings drug resistance spreads faster than in high transmission settings, and treatment failure is the main force driving the spread of drug resistance. In low transmission settings, ACT slows the spread of drug resistance to a partner drug, especially at high coverage rates. This effect decreases exponentially with increasing delay in deploying the ACT and decreasing rates of coverage. In the high transmission settings, however, drug resistance is driven by the proportion of the human population with a residual drug level, which gives resistant parasites some survival advantage. The spread of drug resistance could be slowed down by controlling presumptive drug use and avoiding the use of combination therapies containing drugs with mismatched half-lives, together with reducing malaria transmission through vector control measures.
This paper has demonstrated the use of a comprehensive mathematical model to describe malaria transmission and the spread of drug resistance. The model is strongly linked to the empirical evidence obtained from extensive data available from various sources. This model can be a useful tool to inform the design of treatment policies, particularly at a time when ACT has been endorsed by WHO as first-line treatment for falciparum malaria worldwide.
大多数疟疾流行国家正在将抗疟药物政策转变为以青蒿素为基础的联合疗法(ACT)。不同药物选择和实施策略的影响尚不确定。来自不同疟疾流行程度地区以及耐药性高发地区(如泰国边境)的许多流行病学研究数据无疑具有重要价值。构建一个合适的动态数据驱动模型是定量探索这些策略影响的有力预测工具。
构建了一个综合模型,纳入了人类、蚊子、寄生虫和治疗等重要的流行病学和生物学因素。通过模型开发、确定所需数据和参数化的迭代过程,使模型与实证证据紧密相连。该模型提供了疟疾流行率/发病率和治疗失败等结果的定量指标,并说明了耐药性在低传播和高传播环境中的传播情况。该模型用于评估以ACT应用为重点的不同抗疟政策选项。
该模型有力地预测,在低传播环境中,耐药性传播速度比高传播环境中更快,治疗失败是推动耐药性传播的主要因素。在低传播环境中,ACT减缓了对伙伴药物耐药性的传播,尤其是在高覆盖率情况下。随着ACT部署延迟增加和覆盖率降低,这种效果呈指数下降。然而,在高传播环境中,耐药性由具有残留药物水平的人群比例驱动,这使耐药寄生虫具有一定生存优势。通过控制推定用药、避免使用半衰期不匹配药物的联合疗法以及通过病媒控制措施减少疟疾传播,可以减缓耐药性的传播。
本文展示了使用综合数学模型来描述疟疾传播和耐药性传播。该模型与从各种来源获得的大量数据所得到的实证证据紧密相连。该模型可成为指导治疗政策设计的有用工具,特别是在世卫组织已认可ACT作为全球恶性疟原虫疟疾一线治疗方法之际。