Teboh-Ewungkem Miranda I, Mohammed-Awel Jemal, Baliraine Frederick N, Duke-Sylvester Scott M
Department of Mathematics, Lehigh University, Bethlehem, PA 18015, USA.
Malar J. 2014 Nov 15;13:428. doi: 10.1186/1475-2875-13-428.
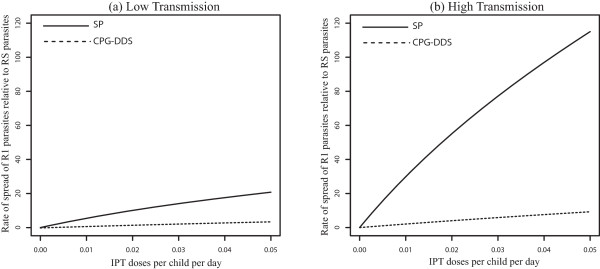
The use of intermittent preventive treatment in pregnant women (IPTp), children (IPTc) and infant (IPTi) is an increasingly popular preventive strategy aimed at reducing malaria risk in these vulnerable groups. Studies to understand how this preventive intervention can affect the spread of anti-malarial drug resistance are important especially when there is human movement between neighbouring low and high transmission areas. Because the same drug is sometimes utilized for IPTi and for symptomatic malaria treatment, distinguishing their individual roles on accelerating the spread of drug resistant malaria, with or without human movement, may be difficult to isolate experimentally or by analysing data. A theoretical framework, as presented here, is thus relevant as the role of IPTi on accelerating the spread of drug resistance can be isolated in individual populations and when the populations are interconnected and interact.
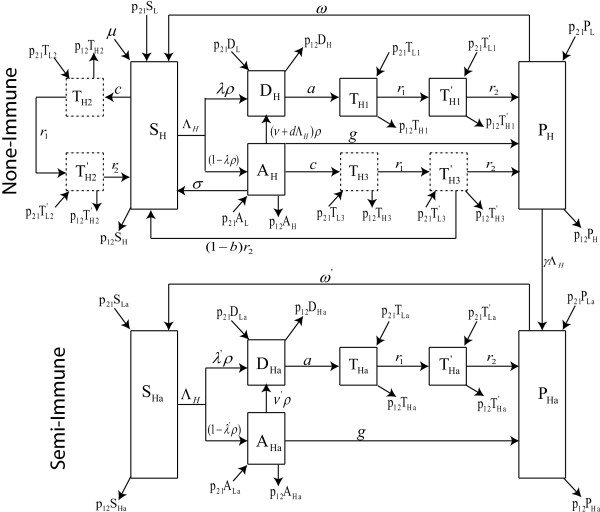
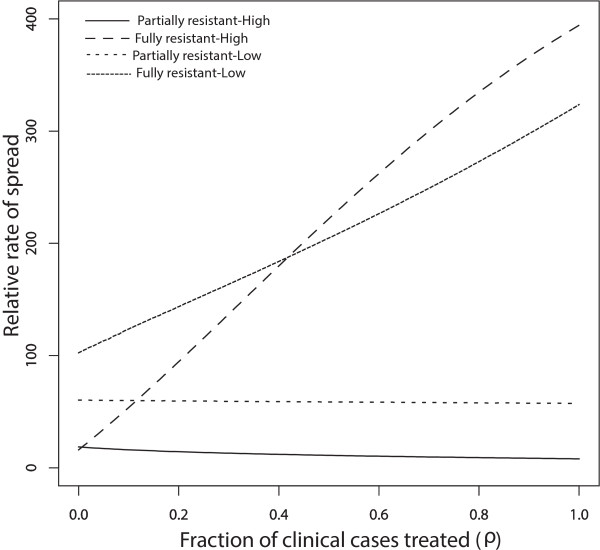
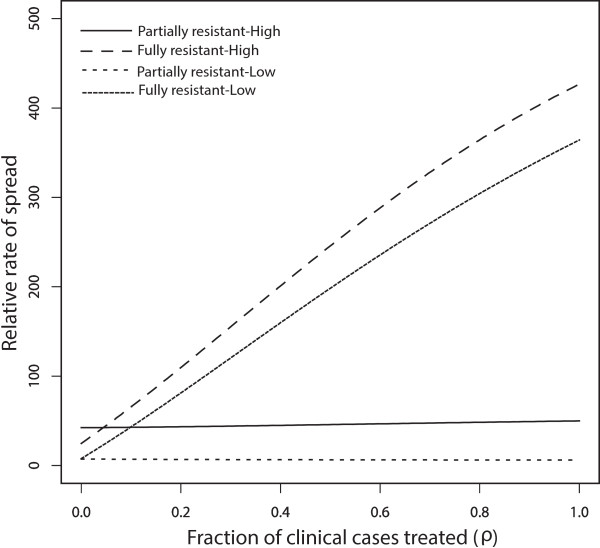
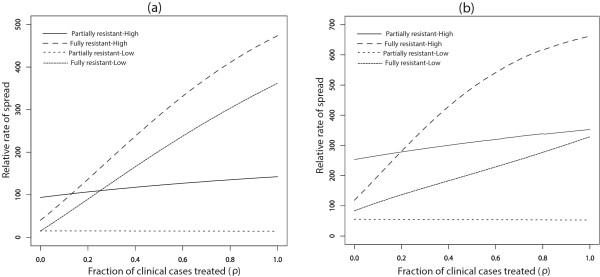
A previously published model is expanded to include human movement between neighbouring high and low transmission areas, with focus placed on the malaria parasites. Parasite fitness functions, determined by how many humans the parasites can infect, are used to investigate how fast resistance can spread within the neighbouring communities linked by movement, when the populations are at endemic equilibrium.
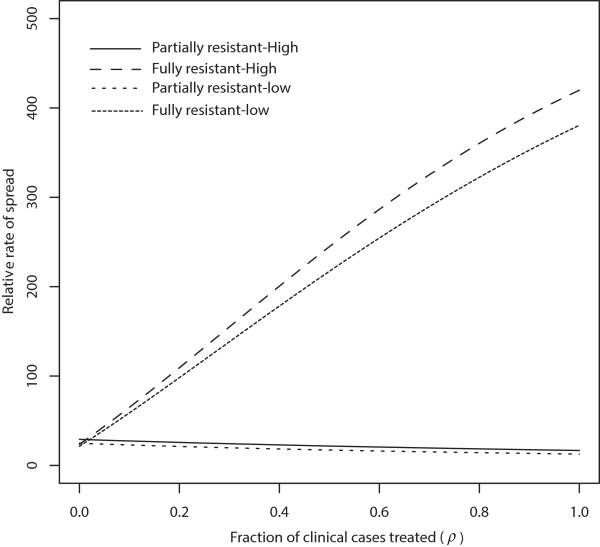
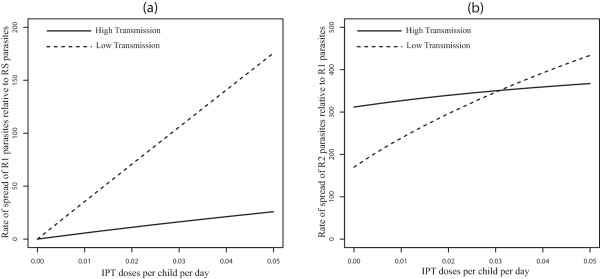
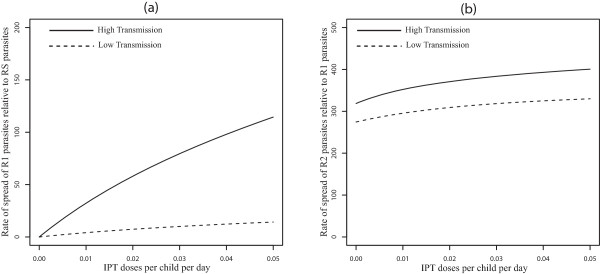
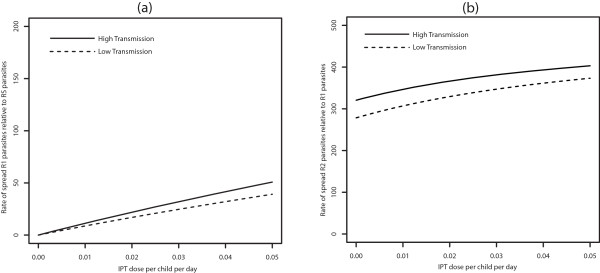
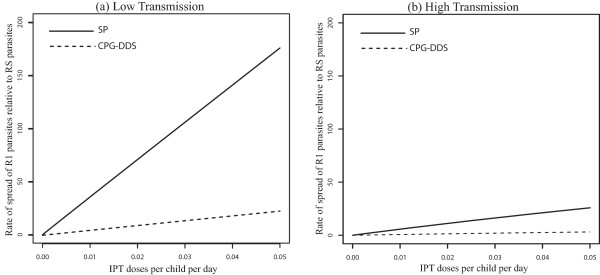
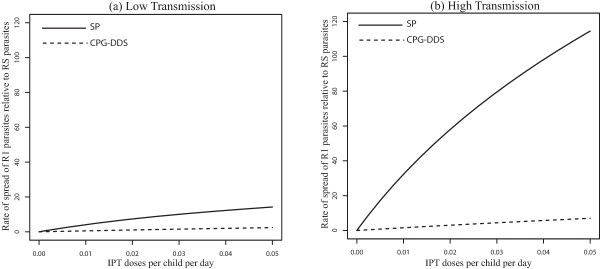
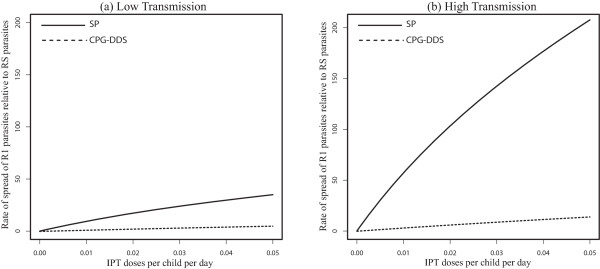
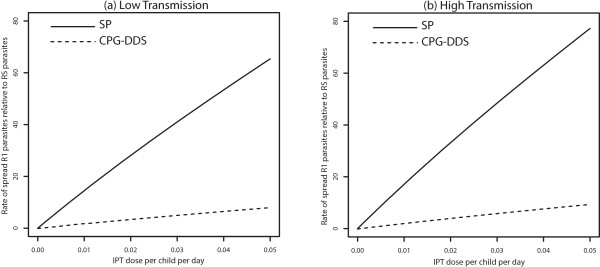
Model simulations indicate that population movement results in resistance spreading fastest in high transmission areas, and the more complete the anti-malarial resistance the faster the resistant parasite will tend to spread through a population. Moreover, the demography of infection in low transmission areas tends to change to reflect the demography of high transmission areas. Additionally, when regions are strongly connected the rate of spread of partially resistant parasites (R1) relative to drug sensitive parasites (RS), and fully resistant parasites (R2) relative to partially resistant parasites (R1) tend to behave the same in both populations, as should be expected.
In fighting anti-malarial drug resistance, different drug resistance monitoring and management policies are needed when the area in question is an isolated high or low transmission area, or when it is close and interacting with a neighbouring high or low transmission area, with human movement between them.
在孕妇(间歇性预防治疗 - 孕妇,IPTp)、儿童(间歇性预防治疗 - 儿童,IPTc)和婴儿(间歇性预防治疗 - 婴儿,IPTi)中使用间歇性预防治疗是一种越来越流行的预防策略,旨在降低这些弱势群体感染疟疾的风险。了解这种预防性干预如何影响抗疟药物耐药性的传播的研究很重要,尤其是当相邻的低传播区和高传播区之间存在人员流动时。由于有时使用相同的药物进行IPTi和症状性疟疾治疗,要区分它们在加速耐药疟疾传播方面的各自作用(无论有无人员流动),可能很难通过实验或数据分析来孤立地确定。因此,本文提出的理论框架具有相关性,因为IPTi在加速耐药性传播方面的作用可以在个体人群中以及当人群相互连接并相互作用时被孤立出来。
对先前发表的模型进行扩展,以纳入相邻高传播区和低传播区之间的人员流动,重点关注疟原虫。通过寄生虫能感染的人类数量确定的寄生虫适应性函数,用于研究在人群处于地方病平衡状态时,耐药性在通过流动连接的相邻社区中传播的速度。
模型模拟表明,人口流动导致耐药性在高传播区传播最快,抗疟耐药性越完全,耐药寄生虫在人群中传播的速度就越快。此外,低传播区的感染人口统计学倾向于发生变化,以反映高传播区的人口统计学。此外,当地区紧密相连时,部分耐药寄生虫(R1)相对于药物敏感寄生虫(RS)的传播速度,以及完全耐药寄生虫(R2)相对于部分耐药寄生虫(R1)的传播速度,在两个群体中往往表现相同,这是可以预期的。
在对抗疟药物耐药性的斗争中,当所讨论的地区是孤立的高传播区或低传播区,或者当它与相邻的高传播区或低传播区接近并相互作用且它们之间存在人员流动时,需要不同的耐药性监测和管理政策。