Buhimschi Irina A, Zhao Guomao, Funai Edmund F, Harris Nathan, Sasson Isaac E, Bernstein Ira M, Saade George R, Buhimschi Catalin S
Department of Obstetrics, Gynecology, and Reproductive Sciences, Yale University School of Medicine, New Haven, CT 06520-8063, USA.
Am J Obstet Gynecol. 2008 Nov;199(5):551.e1-16. doi: 10.1016/j.ajog.2008.07.006.
The cause of preeclampsia remains unknown and the diagnosis can be uncertain. We used proteomic-based analysis of urine to improve disease classification and extend the pathophysiologic understanding of preeclampsia.
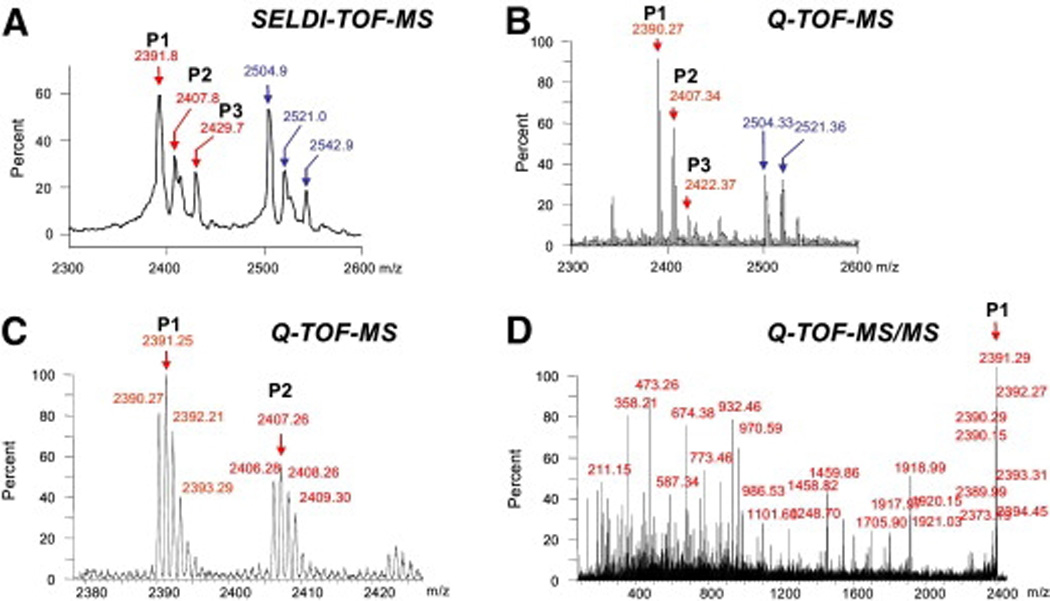
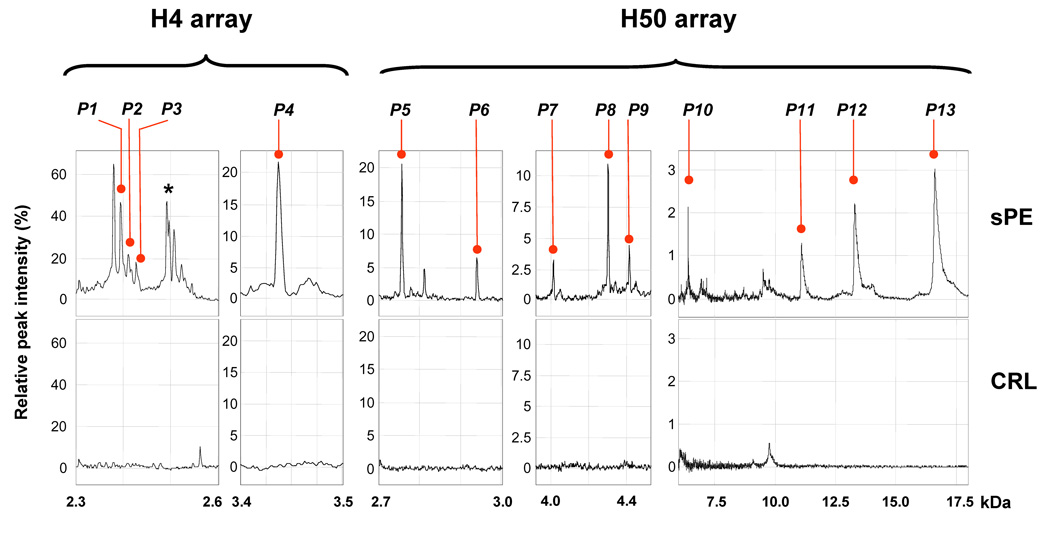
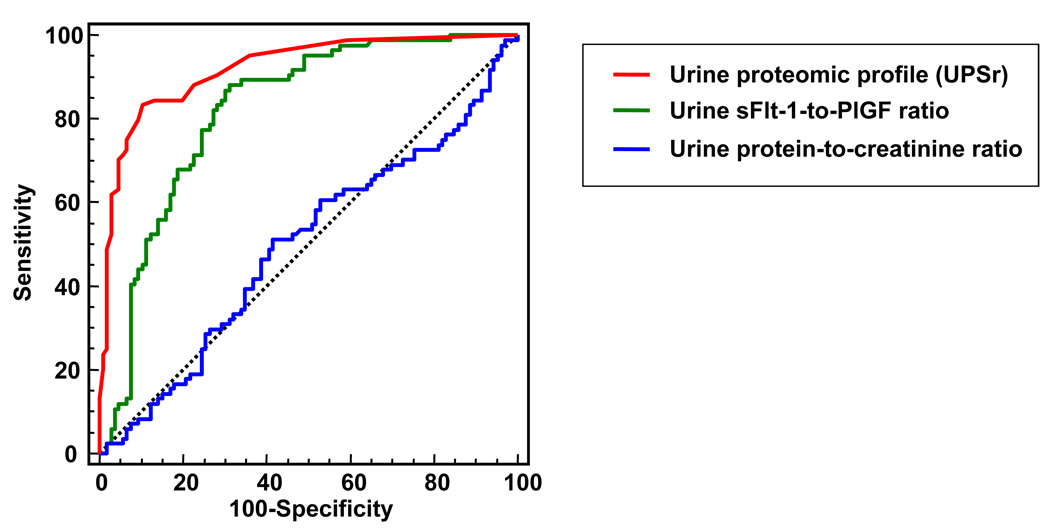
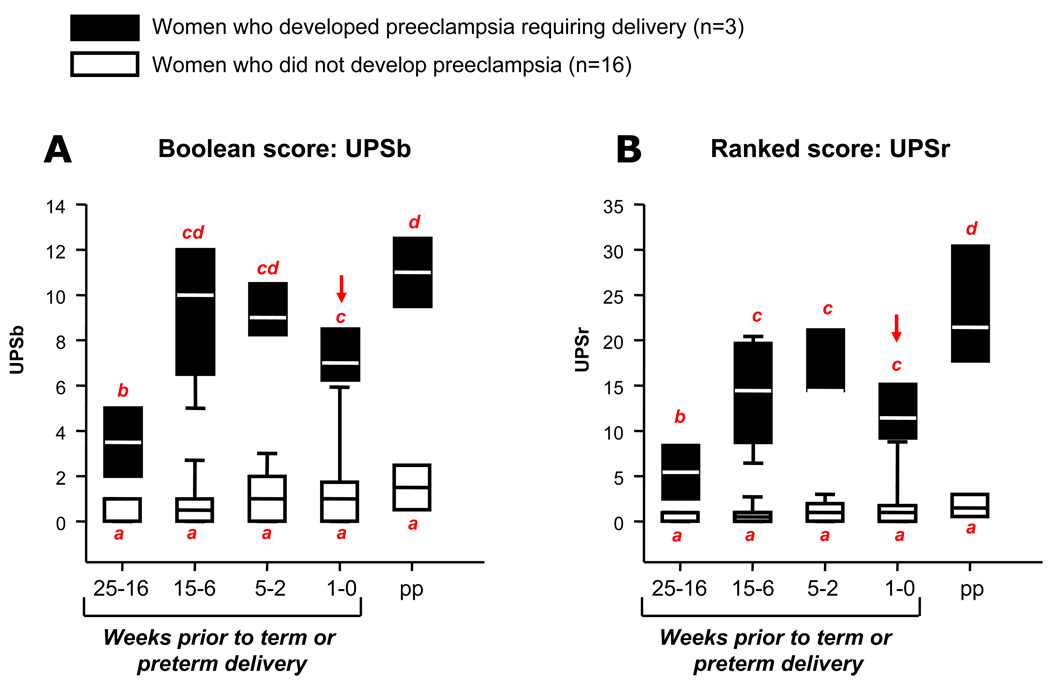
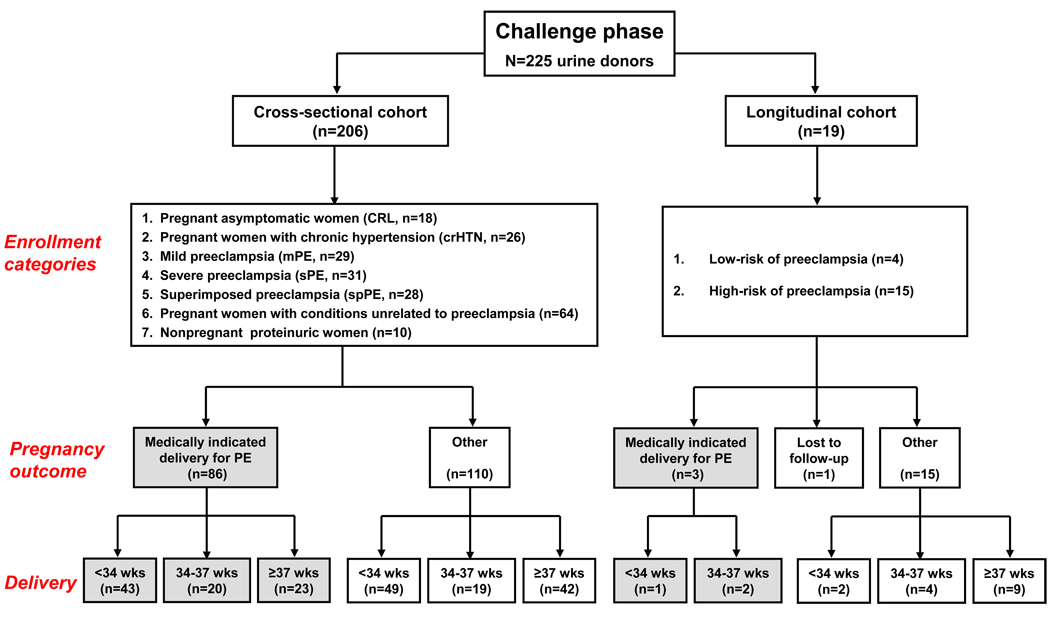
Urine samples from 284 women were analyzed by surface-enhanced laser desorption/ionization. In the exploratory phase, 59 samples were used to extract the proteomic fingerprint characteristic of severe preeclampsia requiring mandated delivery and to develop a diagnostic algorithm. In the challenge phase, we sought to prospectively validate the algorithm in 225 women screened for a variety of high- and low-risk conditions, including preeclampsia. Of these, 19 women were followed longitudinally throughout pregnancy. The presence of biomarkers was interpreted relative to clinical classification, need for delivery, and other urine laboratory measures (ratios of protein to creatinine and soluble fms-like tyrosine kinase-1 to placental growth factor). In the translational phase, biomarker identification by tandem mass spectrometry and validation experiments in urine, serum, and placenta were used to identify, quantify, and localize the biomarkers or related proteins.
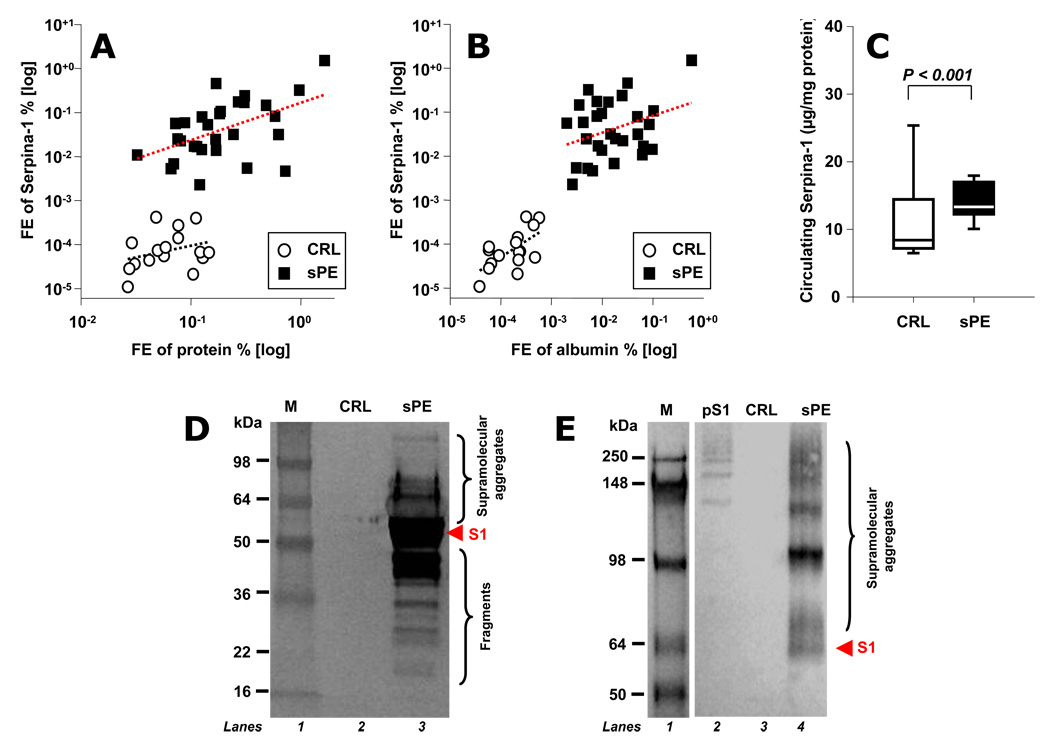
We report that women with preeclampsia appear to present a unique urine proteomic fingerprint that predicts preeclampsia in need of mandated delivery with highest accuracy. This characteristic proteomic profile also has the ability to distinguish preeclampsia from other hypertensive or proteinuric disorders in pregnancy. Pregnant women followed longitudinally who developed preeclampsia displayed abnormal urinary profiles more than 10 weeks before clinical manifestation. Tandem mass spectrometry and de novo sequencing identified the biomarkers as nonrandom cleavage products of SERPINA1 and albumin. Of these, the 21 amino acid C-terminus fragment of SERPINA1 was highly associated with severe forms of preeclampsia requiring early delivery. In preeclampsia, increased and aberrant SERPINA1 immunoreactivity was found in urine, serum, and placenta, in which it localized predominantly to placental villi and placental vascular spaces adherent to the endothelium. In addition, significant perivascular deposits of misfolded SERPINA1 aggregates were exclusively identified in preeclamptic placentae.
Proteomics-based characterization of urine in preeclampsia identified a proteomic fingerprint composed of SERPINA1 and albumin fragments, which can accurately diagnose preeclampsia and shows promise to discriminate it from other hypertensive proteinuric diseases. These findings provide insight into a novel pathophysiological mechanism of preeclampsia related to SERPINA1 misfolding, which may offer new therapeutic opportunities in the future.
子痫前期的病因尚不清楚,诊断也可能存在不确定性。我们采用基于蛋白质组学的尿液分析方法来改善疾病分类,并拓展对子痫前期病理生理学的认识。
采用表面增强激光解吸/电离技术对284名女性的尿液样本进行分析。在探索阶段,使用59个样本提取需要强制分娩的重度子痫前期的蛋白质组指纹特征,并开发一种诊断算法。在验证阶段,我们试图在前瞻性地对225名接受各种高风险和低风险状况筛查的女性(包括子痫前期患者)中验证该算法。其中,19名女性在整个孕期接受纵向随访。根据临床分类、分娩需求以及其他尿液实验室指标(蛋白质与肌酐的比值以及可溶性fms样酪氨酸激酶-1与胎盘生长因子的比值)来解读生物标志物的存在情况。在转化阶段,通过串联质谱法鉴定生物标志物,并在尿液、血清和胎盘中进行验证实验,以识别、定量和定位生物标志物或相关蛋白质。
我们报告称,子痫前期女性似乎呈现出一种独特的尿液蛋白质组指纹,能够以最高的准确性预测需要强制分娩的子痫前期。这种特征性蛋白质组图谱还能够将子痫前期与妊娠期间的其他高血压或蛋白尿性疾病区分开来。纵向随访中发生子痫前期的孕妇在临床表现出现前10周以上就显示出异常的尿液图谱。串联质谱法和从头测序确定生物标志物为丝氨酸蛋白酶抑制剂A1(SERPINA1)和白蛋白的非随机裂解产物。其中,SERPINA1的21个氨基酸C末端片段与需要早期分娩的重度子痫前期密切相关。在子痫前期患者的尿液、血清和胎盘中发现SERPINA1的免疫反应性增加且异常,其主要定位于胎盘绒毛和附着于内皮的胎盘血管间隙。此外,仅在子痫前期胎盘中发现了错误折叠的SERPINA1聚集体的显著血管周围沉积。
基于蛋白质组学的子痫前期尿液特征分析确定了一种由SERPINA1和白蛋白片段组成的蛋白质组指纹,它能够准确诊断子痫前期,并有望将其与其他高血压蛋白尿性疾病区分开来。这些发现为子痫前期与SERPINA1错误折叠相关的新病理生理机制提供了见解,这可能在未来提供新的治疗机会。