Hull Sara Chandros, Sharp Richard R, Botkin Jeffrey R, Brown Mark, Hughes Mark, Sugarman Jeremy, Schwinn Debra, Sankar Pamela, Bolcic-Jankovic Dragana, Clarridge Brian R, Wilfond Benjamin S
National Human Genome Research Institute, National Institutes of Health, Bethesda, MD 20892-1156, USA.
Am J Bioeth. 2008 Oct;8(10):62-70. doi: 10.1080/15265160802478404.
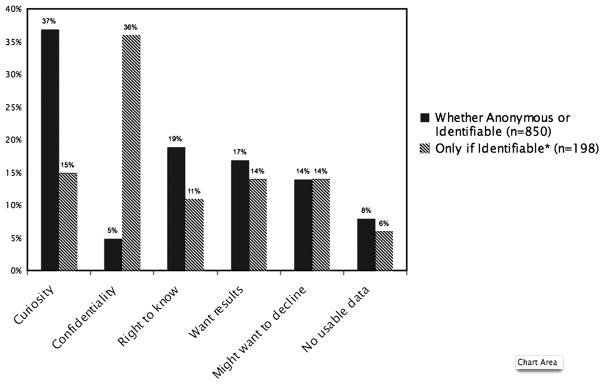
It is unclear whether the regulatory distinction between non-identifiable and identifiable information--information used to determine informed consent practices for the use of clinically derived samples for genetic research--is meaningful to patients. The objective of this study was to examine patients' attitudes and preferences regarding use of anonymous and identifiable clinical samples for genetic research. Telephone interviews were conducted with 1,193 patients recruited from general medicine, thoracic surgery, or medical oncology clinics at five United States academic medical centers. Wanting to know about research being done was important to 72% of patients when samples would be anonymous and to 81% of patients when samples would be identifiable. Only 17% wanted to know about the identifiable scenario but not the anonymous scenario (i.e., following the regulatory distinction). Curiosity-based reasons were the most common (37%) among patients who wanted to know about anonymous samples. Of patients wanting to know about either scenario, approximately 57% would require researchers to seek permission, whereas 43% would be satisfied with notification only. Patients were more likely to support permission (versus notification) in the anonymous scenario if they had more education, were Black, less religious, in better health, more private, and less trusting of researchers. The sample, although not representative of the general population, does represent patients at academic medical centers whose clinical samples may be used for genetic research. Few patients expressed preferences consistent with the regulatory distinction between non-identifiable and identifiable information. Data from this study should cause policy-makers to question whether this distinction is useful in relation to research with previously collected clinically derived samples.
目前尚不清楚不可识别信息与可识别信息之间的监管区别(用于确定将临床来源样本用于基因研究的知情同意做法的信息)对患者是否有意义。本研究的目的是调查患者对于将匿名和可识别临床样本用于基因研究的态度和偏好。对从美国五家学术医疗中心的普通内科、胸外科或医学肿瘤学诊所招募的1193名患者进行了电话访谈。当样本为匿名时,72%的患者认为了解正在进行的研究很重要;当样本为可识别时,这一比例为81%。只有17%的患者想了解可识别情况但不想了解匿名情况(即遵循监管区别)。在想了解匿名样本的患者中,基于好奇心的原因最为常见(37%)。在想了解任何一种情况的患者中,约57%的患者要求研究人员寻求许可,而43%的患者仅接受通知就会满意。如果患者受教育程度更高、为黑人、宗教信仰较少、健康状况更好、更注重隐私且对研究人员的信任度较低,那么他们在匿名情况下更有可能支持寻求许可(而非仅接受通知)。该样本虽然不代表一般人群,但确实代表了学术医疗中心的患者,其临床样本可能会用于基因研究。很少有患者表达出与不可识别信息和可识别信息之间的监管区别一致的偏好。本研究的数据应促使政策制定者质疑这种区别对于使用先前收集的临床来源样本进行的研究是否有用。