Wolfe Frederick, Petri Michelle, Alarcón Graciela S, Goldman John, Chakravarty Eliza F, Katz Robert S, Karlson Elizabeth W
National Data Bank for Rheumatic Diseases, 1035 N. Emporia, Suite 288, Wichita, KS 67214, USA.
J Rheumatol. 2009 Jan;36(1):82-8. doi: 10.3899/jrheum.080212.
To determine if fibromyalgia (FM) or fibromyalgia-ness (the tendency to respond to illness and psychosocial stress with fatigue, widespread pain, general increase in symptoms, and similar factors) is increased in patients with compared to those without systemic lupus erythematosus (SLE); to determine whether FM or fibromyalgia-ness biases the SLE Activity Questionnaire (SLAQ); and to determine if the SLAQ is overly sensitive to FM symptoms.
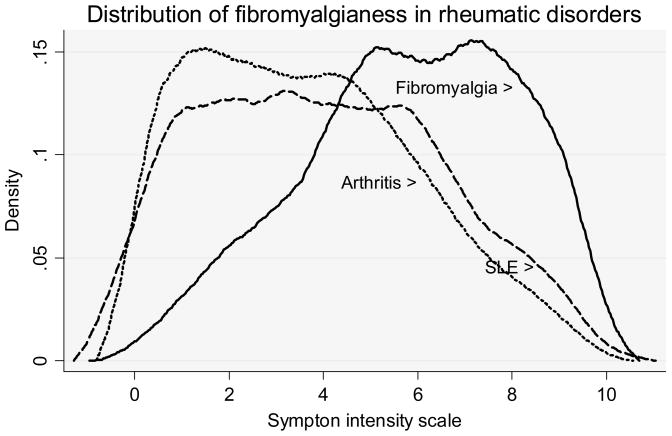
We developed a 16-item SLE Symptom Scale (SLESS) modeled on the SLAQ and used that scale to investigate the relation between SLE symptoms and fibromyalgia-ness in 23,321 patients with rheumatic disease. FM was diagnosed by survey FM criteria, and fibromyalgia-ness was measured using the Symptom Intensity (SI) Scale. As comparison groups, we combined patients with rheumatoid arthritis and noninflammatory rheumatic disorders into an "arthritis" group and also utilized a physician-diagnosed group of patients with FM.
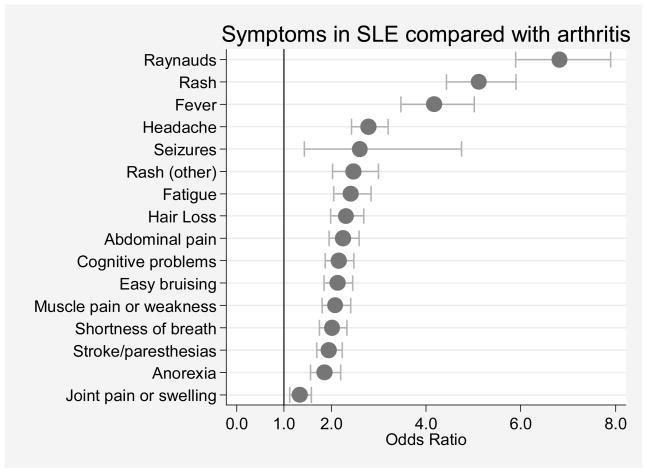
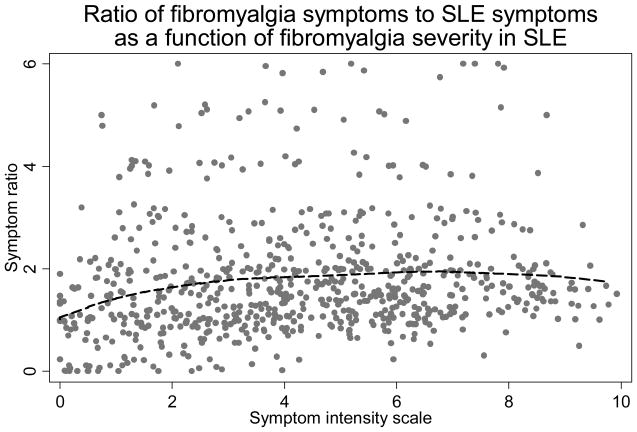
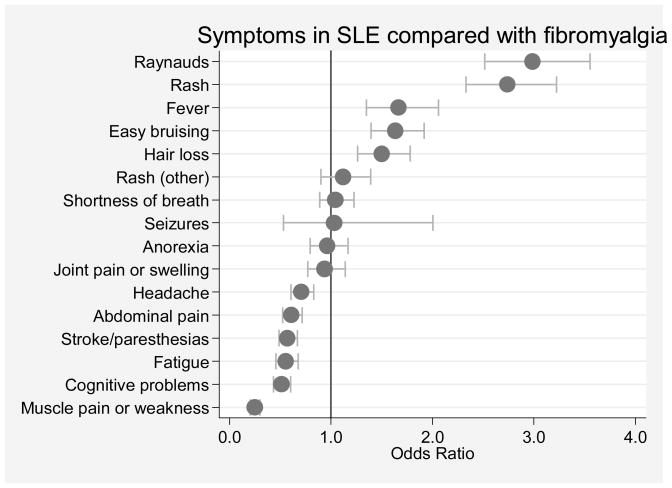
FM was identified in 22.1% of SLE and 17.0% of those with arthritis. The SI scale was minimally increased in SLE. The correlation between SLAQ and SLESS was 0.738. SLESS/SLAQ scale items (Raynaud's phenomenon, rash, fever, easy bruising, hair loss) were significantly more associated with SLE than FM, while the reverse was true for headache, abdominal pain, paresthesias/stroke, fatigue, cognitive problems, and muscle pain or weakness. There was no evidence of disproportionate symptom-reporting associated with fibromyalgia-ness. Self-reported SLE was associated with an increased prevalence of FM that was unconfirmed by physicians, compared to SLE confirmed by physicians.
The prevalence of FM in SLE is minimally increased compared with its prevalence in patients with arthritis. Fibromyalgia-ness does not bias the SLESS and should not bias SLE assessments, including the SLAQ.
确定与无系统性红斑狼疮(SLE)的患者相比,SLE患者的纤维肌痛(FM)或纤维肌痛倾向(即对疾病和心理社会压力产生疲劳、广泛疼痛、症状普遍加重及类似因素的倾向)是否增加;确定FM或纤维肌痛倾向是否会影响SLE活动问卷(SLAQ);以及确定SLAQ对FM症状是否过度敏感。
我们以SLAQ为蓝本制定了一个包含16个项目的SLE症状量表(SLESS),并用该量表调查了23321例风湿病患者中SLE症状与纤维肌痛倾向之间的关系。通过调查FM标准诊断FM,使用症状强度(SI)量表测量纤维肌痛倾向。作为对照组,我们将类风湿关节炎患者和非炎性风湿性疾病患者合并为一个“关节炎”组,同时还使用了医生诊断的FM患者组。
在SLE患者中,22.1%被诊断为FM,在关节炎患者中这一比例为17.0%。SI量表在SLE患者中的升高幅度极小。SLAQ与SLESS之间的相关性为0.738。SLESS/SLAQ量表项目(雷诺现象、皮疹、发热、易瘀伤、脱发)与SLE的相关性显著高于与FM的相关性,而对于头痛、腹痛、感觉异常/中风、疲劳、认知问题以及肌肉疼痛或无力,情况则相反。没有证据表明存在与纤维肌痛倾向相关的不成比例的症状报告。与医生确诊的SLE相比,自我报告的SLE患者中FM患病率增加,但未得到医生的证实。
与关节炎患者相比,SLE患者中FM的患病率略有增加。纤维肌痛倾向不会影响SLESS,也不应影响包括SLAQ在内的SLE评估。