Swanson Kristin R, Chakraborty Gargi, Wang Christina H, Rockne Russell, Harpold Hana L P, Muzi Mark, Adamsen Tom C H, Krohn Kenneth A, Spence Alexander M
Department of Pathology, University of Washington, Seattle, Washington 98195, USA.
J Nucl Med. 2009 Jan;50(1):36-44. doi: 10.2967/jnumed.108.055467. Epub 2008 Dec 17.
Glioblastoma multiforme is a primary brain tumor known for its rapid proliferation, diffuse invasion, and prominent neovasculature and necrosis. This study explores the in vivo link between these characteristics and hypoxia by comparing the relative spatial geometry of developing vasculature inferred from gadolinium-enhanced T1-weighted MRI (T1Gd), edematous tumor extent revealed on T2-weighted MRI (T2), and hypoxia assessed by 18F-fluoromisonidazole PET (18F-FMISO). Given the role of hypoxia in upregulating angiogenic factors, we hypothesized that the distribution of hypoxia seen on 18F-FMISO is correlated spatially and quantitatively with the amount of leaky neovasculature seen on T1Gd.
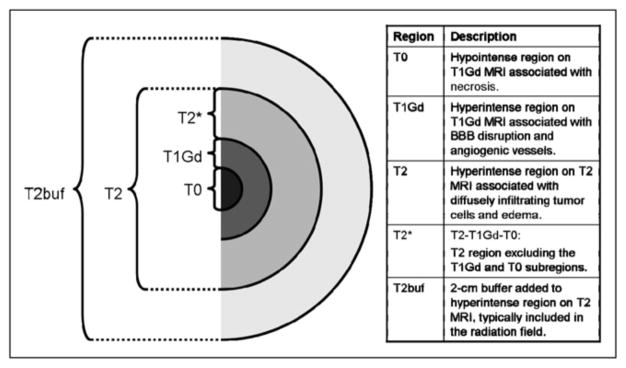
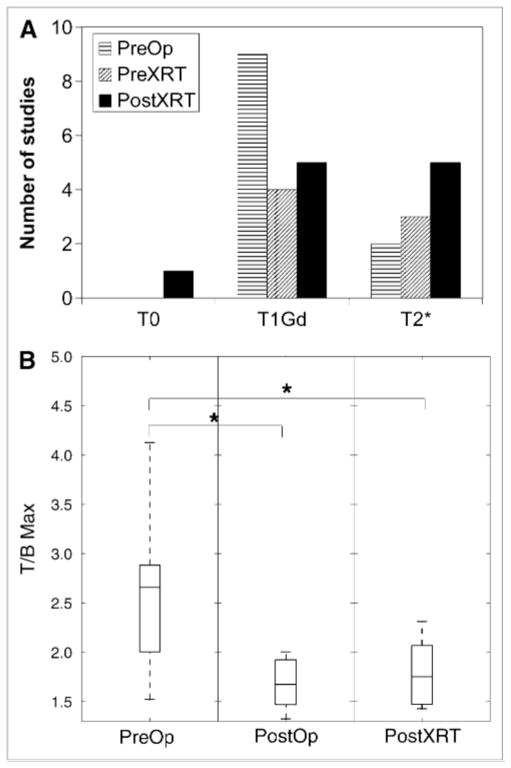
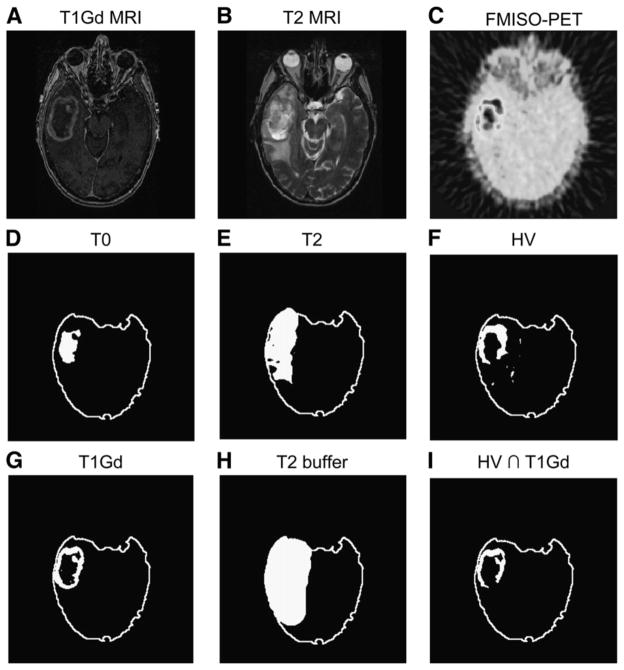
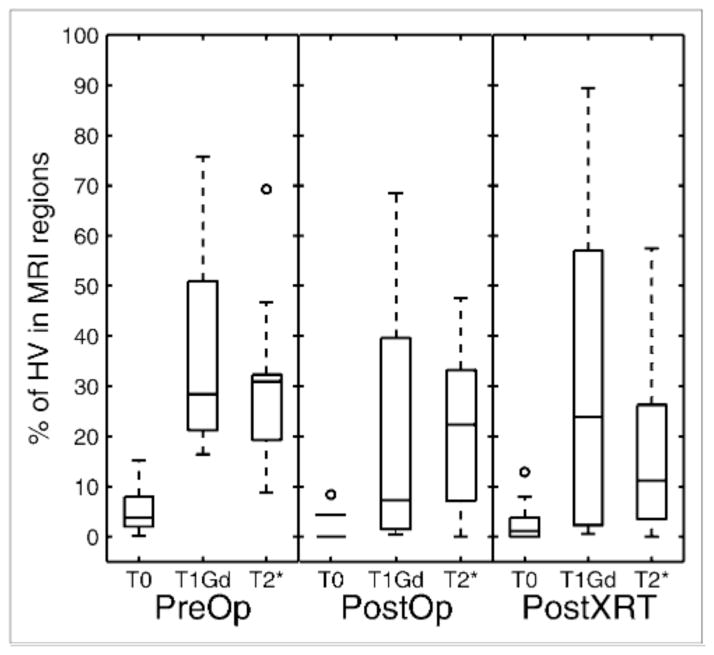
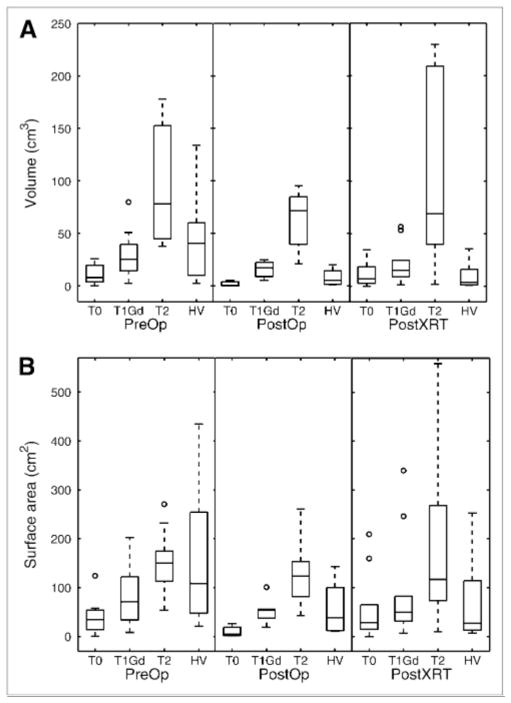
A total of 24 patients with glioblastoma underwent T1Gd, T2, and 18F-FMISO-11 studies preceded surgical resection or biopsy, 7 followed surgery and preceded radiation therapy, and 11 followed radiation therapy. Abnormal regions seen on the MRI scan were segmented, including the necrotic center (T0), the region of abnormal blood-brain barrier associated with disrupted vasculature (T1Gd), and infiltrating tumor cells and edema (T2). The 18F-FMISO images were scaled to the blood 18F-FMISO activity to create tumor-to-blood ratio (T/B) images. The hypoxic volume (HV) was defined as the region with T/Bs greater than 1.2, and the maximum T/B (T/Bmax) was determined by the voxel with the greatest T/B value.
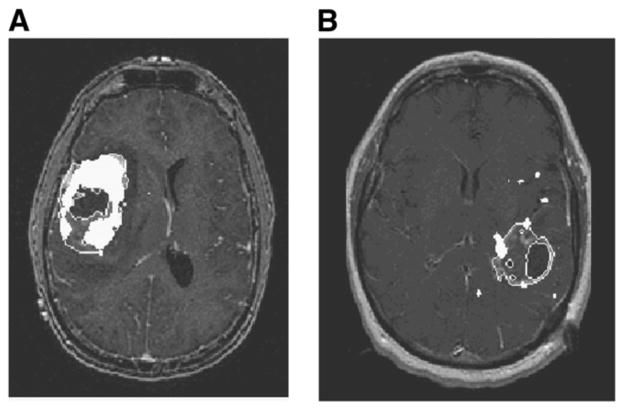
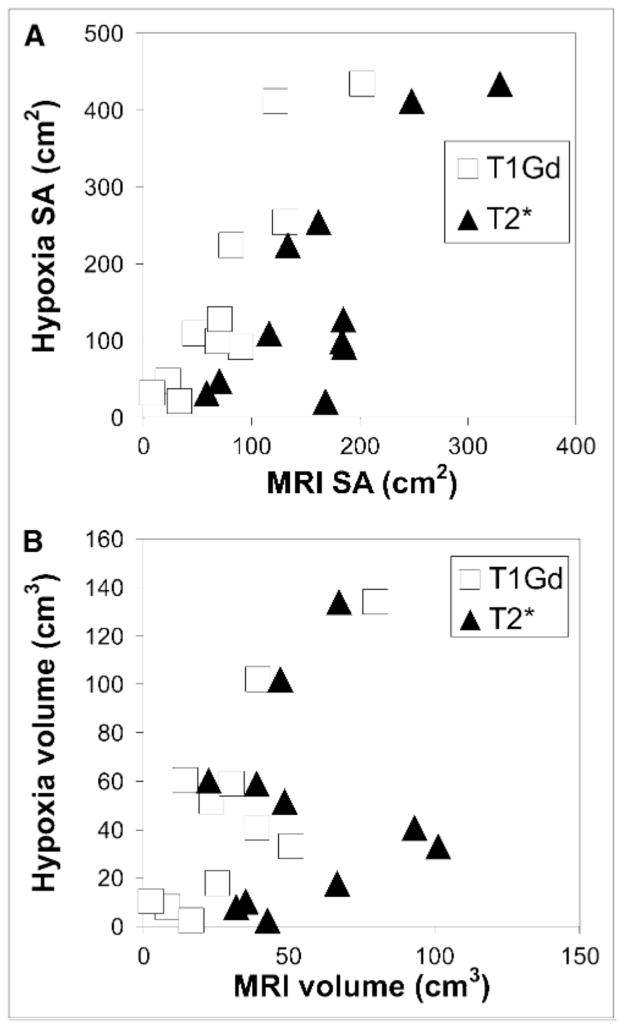
The HV generally occupied a region straddling the outer edge of the T1Gd abnormality and into the T2. A significant correlation between HV and the volume of the T1Gd abnormality that relied on the existence of a large outlier was observed. However, there was consistent correlation between surface areas of all MRI-defined regions and the surface area of the HV. The T/Bmax, typically located within the T1Gd region, was independent of the MRI-defined tumor size. Univariate survival analysis found the most significant predictors of survival to be HV, surface area of HV, surface area of T1Gd, and T/Bmax.
Hypoxia may drive the peripheral growth of glioblastomas. This conclusion supports the spatial link between the volumes and surface areas of the hypoxic and MRI regions; the magnitude of hypoxia, T/Bmax, remains independent of size.
多形性胶质母细胞瘤是一种原发性脑肿瘤,以其快速增殖、弥漫性侵袭、显著的新生血管形成和坏死为特征。本研究通过比较钆增强T1加权磁共振成像(T1Gd)推断的发育中血管的相对空间几何结构、T2加权磁共振成像(T2)显示的水肿性肿瘤范围以及18F-氟米索硝唑正电子发射断层扫描(18F-FMISO)评估的缺氧情况,探讨了这些特征与缺氧之间的体内联系。鉴于缺氧在上调血管生成因子中的作用,我们假设18F-FMISO上所见缺氧的分布在空间和数量上与T1Gd上所见渗漏性新生血管的数量相关。
共有24例胶质母细胞瘤患者在手术切除或活检前接受了T1Gd、T2和18F-FMISO-11检查,7例在手术后放疗前接受检查,11例在放疗后接受检查。对MRI扫描上看到的异常区域进行分割,包括坏死中心(T0)、与血管破坏相关的血脑屏障异常区域(T1Gd)以及浸润性肿瘤细胞和水肿(T2)。将18F-FMISO图像按血液18F-FMISO活性进行缩放,以创建肿瘤与血液比值(T/B)图像。缺氧体积(HV)定义为T/B大于1.2的区域,最大T/B(T/Bmax)由T/B值最大的体素确定。
HV通常占据跨越T1Gd异常外边缘并延伸至T2的区域。观察到HV与T1Gd异常体积之间存在显著相关性,该相关性依赖于一个大的离群值的存在。然而,所有MRI定义区域的表面积与HV的表面积之间存在一致的相关性。T/Bmax通常位于T1Gd区域内,与MRI定义的肿瘤大小无关。单因素生存分析发现,生存的最显著预测因素是HV、HV的表面积、T1Gd的表面积和T/Bmax。
缺氧可能驱动胶质母细胞瘤的外周生长。这一结论支持了缺氧区域和MRI区域的体积与表面积之间的空间联系;缺氧程度T/Bmax与大小无关。