Zhang Min, Holman C D'Arcy J, Price Sylvie D, Sanfilippo Frank M, Preen David B, Bulsara Max K
School of Population Health, University of Western Australia, Perth, WA, Australia.
BMJ. 2009 Jan 7;338:a2752. doi: 10.1136/bmj.a2752.
To identify factors that predict repeat admission to hospital for adverse drug reactions (ADRs) in older adults.
Population based retrospective cohort study.
All public and private hospitals in Western Australia.
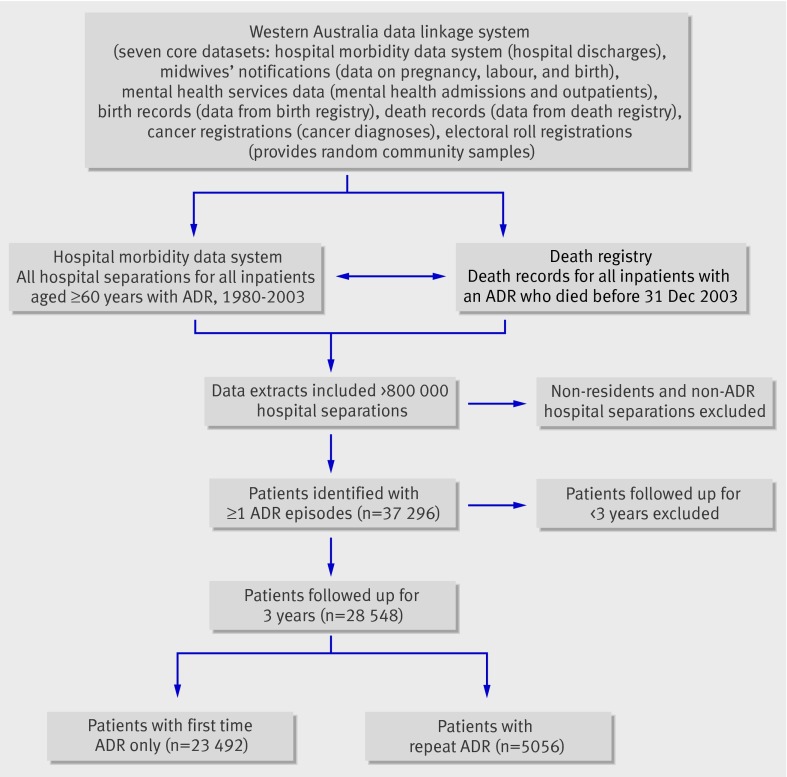
28 548 patients aged >or=60 years with an admission for an ADR during 1980-2000 followed for three years using the Western Australian data linkage system.
5056 (17.7%) patients had a repeat admission for an ADR. Repeat ADRs were associated with sex (hazard ratio 1.08, 95% confidence interval 1.02 to 1.15, for men), first admission in 1995-9 (2.34, 2.00 to 2.73), length of hospital stay (1.11, 1.05 to 1.18, for stays >or=14 days), and Charlson comorbidity index (1.71, 1.46 to 1.99, for score >or=7); 60% of comorbidities were recorded and taken into account in analysis. In contrast, advancing age had no effect on repeat ADRs. Comorbid congestive cardiac failure (1.56, 1.43 to 1.71), peripheral vascular disease (1.27, 1.09 to 1.48), chronic pulmonary disease (1.61, 1.45 to 1.79), rheumatological disease (1.65, 1.41 to 1.92), mild liver disease (1.48, 1.05 to 2.07), moderate to severe liver disease (1.85, 1.18 to 2.92), moderate diabetes (1.18, 1.07 to 1.30), diabetes with chronic complications (1.91, 1.65 to 2.22), renal disease (1.93, 1.71 to 2.17), any malignancy including lymphoma and leukaemia (1.87, 1.68 to 2.09), and metastatic solid tumours (2.25, 1.92 to 2.64) were strong predictive factors. Comorbidities requiring continuing care predicted a reduced likelihood of repeat hospital admissions for ADRs (cerebrovascular disease 0.85, 0.73 to 0.98; dementia 0.62, 0.49 to 0.78; paraplegia 0.73, 0.59 to 0.89).
Comorbidity, but not advancing age, predicts repeat admission for ADRs in older adults, especially those with comorbidities often managed in the community. Awareness of these predictors can help clinicians to identify which older adults are at greater risk of admission for ADRs and, therefore, who might benefit from closer monitoring.
确定预测老年患者因药物不良反应(ADR)再次入院的因素。
基于人群的回顾性队列研究。
西澳大利亚州的所有公立和私立医院。
1980年至2000年间因ADR入院的28548名年龄≥60岁的患者,使用西澳大利亚数据链接系统随访三年。
5056名(17.7%)患者因ADR再次入院。再次发生ADR与性别(男性风险比1.08,95%置信区间1.02至1.15)、1995年至1999年首次入院(2.34,2.00至2.73)、住院时间(住院≥14天者为1.11,1.05至1.18)以及查尔森合并症指数(得分≥7者为1.71,1.46至1.99)相关;60%的合并症在分析中被记录并纳入考虑。相比之下,年龄增长对再次发生ADR没有影响。合并充血性心力衰竭(1.56,1.43至1.71)、外周血管疾病(1.27,1.09至1.48)、慢性肺病(1.61,1.45至1.79)、风湿性疾病(1.65,1.41至1.92)、轻度肝病(1.48,1.05至2.07)、中度至重度肝病(1.85,1.18至2.92)、中度糖尿病(1.18,1.07至1.30)、伴有慢性并发症的糖尿病(1.91,1.65至2.22)、肾病(1.93,1.71至2.17)、任何恶性肿瘤包括淋巴瘤和白血病(1.87,1.68至2.09)以及转移性实体瘤(2.25,1.92至2.64)是强烈的预测因素。需要持续护理的合并症预测因ADR再次住院的可能性降低(脑血管疾病0.85,0.73至0.98;痴呆0.62,0.49至0.78;截瘫0.73,0.59至0.89)。
合并症而非年龄增长可预测老年患者因ADR再次入院,尤其是那些合并症常在社区管理的患者。了解这些预测因素有助于临床医生识别哪些老年患者因ADR入院风险更高,从而确定哪些患者可能从更密切的监测中获益。