Richardson Gerry, Bloor Karen, Williams John, Russell Ian, Durai Dharmaraj, Cheung Wai Yee, Farrin Amanda, Coulton Simon
Centre for Health Economics and Hull York Medical School (HYMS), University of York, York YO10 5DD.
BMJ. 2009 Feb 10;338:b270. doi: 10.1136/bmj.b270.
To compare the cost effectiveness of nurses and doctors in performing upper gastrointestinal endoscopy and flexible sigmoidoscopy.
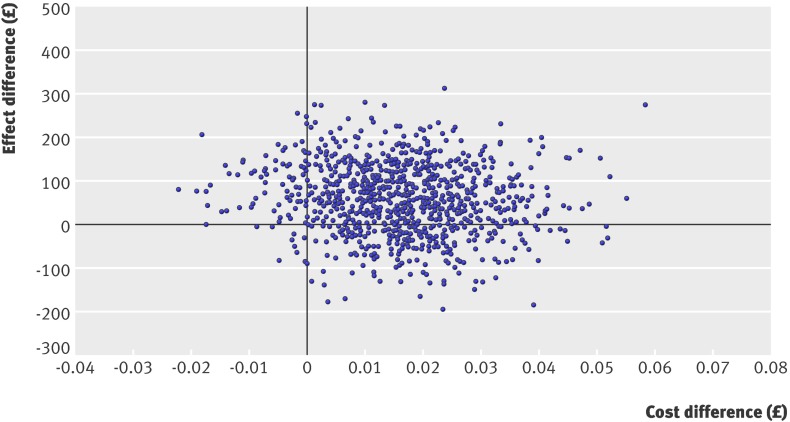
As part of a pragmatic randomised trial, the economic analysis calculated incremental cost effectiveness ratios, and generated cost effectiveness acceptability curves to address uncertainty.
23 hospitals in the United Kingdom.
67 doctors and 30 nurses, with a total of 1888 patients, from July 2002 to June 2003.
Diagnostic upper gastrointestinal endoscopy and flexible sigmoidoscopy carried out by doctors or nurses.
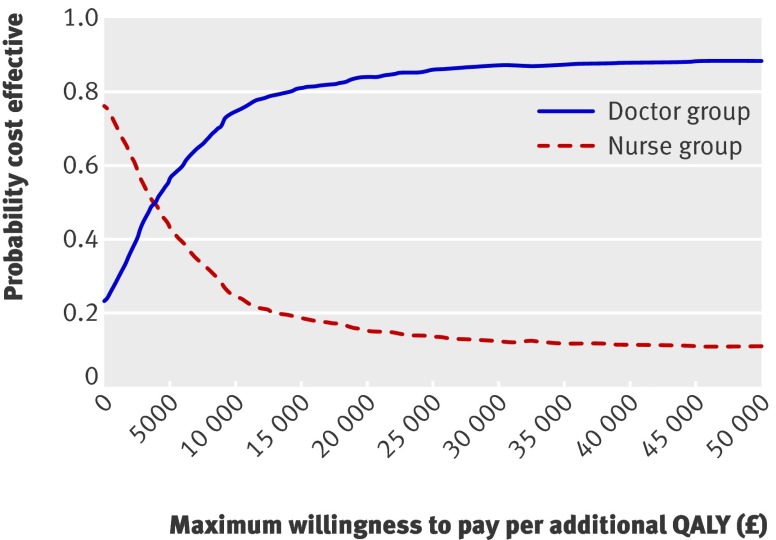
Estimated health gains in QALYs measured with EQ-5D. Probability of cost effectiveness over a range of decision makers' willingness to pay for an additional quality adjusted life year (QALY).
Although differences did not reach traditional levels of significance, patients in the doctor group gained 0.015 QALYs more than those in the nurse group, at an increased cost of about pound56 (euro59, $78) per patient. This yields an incremental cost effectiveness ratio of pound3660 (euro3876, $5097) per QALY. Though there is uncertainty around these results, doctors are probably more cost effective than nurses for plausible values of a QALY.
Though upper gastrointestinal endoscopies and flexible sigmoidoscopies carried out by doctors cost slightly more than those by nurses and improved health outcomes only slightly, our analysis favours endoscopies by doctors. For plausible values of decision makers' willingness to pay for an extra QALY, endoscopy delivered by nurses is unlikely to be cost effective compared with endoscopy delivered by doctors.
International standard RCT 82765705.
比较护士和医生进行上消化道内镜检查及乙状结肠镜检查的成本效益。
作为一项实用随机试验的一部分,经济分析计算了增量成本效益比,并生成成本效益可接受性曲线以应对不确定性。
英国23家医院。
2002年7月至2003年6月期间的67名医生和30名护士,共1888名患者。
由医生或护士进行诊断性上消化道内镜检查及乙状结肠镜检查。
用EQ-5D测量以质量调整生命年(QALY)衡量的估计健康收益。在一系列决策者为额外一个质量调整生命年(QALY)的支付意愿范围内的成本效益概率。
尽管差异未达到传统的显著水平,但医生组患者比护士组患者多获得0.015个QALY,每位患者成本增加约56英镑(59欧元,78美元)。这产生了每QALY 3660英镑(3876欧元,5097美元)的增量成本效益比。尽管这些结果存在不确定性,但对于QALY的合理值,医生可能比护士更具成本效益性。
尽管医生进行的上消化道内镜检查和乙状结肠镜检查比护士进行的成本略高,且健康结果改善仅略有增加,但我们的分析支持由医生进行内镜检查。对于决策者为额外一个QALY的合理支付意愿值,与医生进行的内镜检查相比,护士进行的内镜检查不太可能具有成本效益性。
国际标准随机对照试验82765705 。