Clough Geraldine F, Turzyniecka Magdalena, Walter Lara, Krentz Andrew J, Wild Sarah H, Chipperfield Andrew J, Gamble John, Byrne Christopher D
School of Medicine, University of Southampton, Southampton, UK.
Diabetes. 2009 May;58(5):1185-91. doi: 10.2337/db08-1688. Epub 2009 Feb 10.
To test the hypotheses that decreased insulin-mediated glucose disposal in muscle is associated with a reduced muscle microvascular exchange capacity (Kf) and that 6 months of high-dose statin therapy would improve microvascular function in people with central obesity.
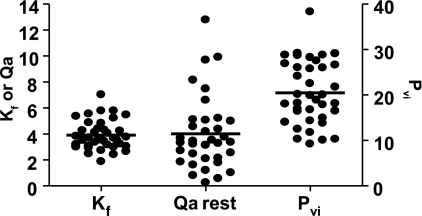
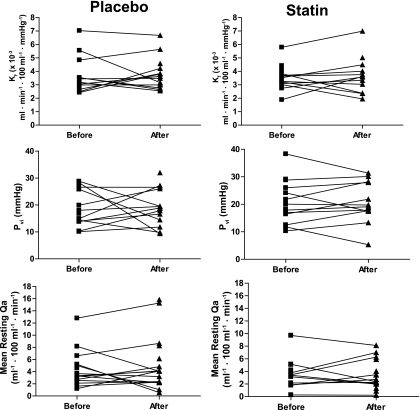
We assessed skeletal muscle microvascular function, visceral fat mass, physical activity levels, fitness, and insulin sensitivity in skeletal muscle in 22 female and 17 male volunteers with central obesity whose age (mean +/- SD) was 51 +/- 9 years. We tested the effect of atorvastatin (40 mg daily) on muscle microvascular function in a randomized, double-blind, placebo-controlled trial lasting 6 months.
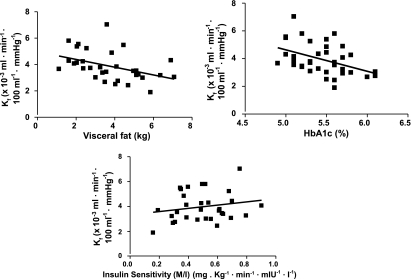
Kf was negatively associated with a measure of glycemia (A1C; r = -0.44, P = 0.006) and positively associated with insulin sensitivity (the ratio of insulin-stimulated glucose effectiveness, or M value, to the mean insulin concentration, or I value; r = 0.39, P = 0.02). In regression modeling, A1C, visceral fat mass, and M:I explained 38% of the variance in Kf (in a linear regression model with Kf as the outcome [R2 = 0.38, P = 0.005]). M:I was associated with Kf independently of visceral fat mass (B coefficient 3.13 [95% CI 0.22-6.02], P = 0.036). Although 6 months' treatment with atorvastatin decreased LDL cholesterol by 51% (P < 0.001) and plasma high-sensitivity C-reactive protein by 75% (P = 0.02), microvascular function was unchanged.
Decreased insulin-mediated glucose uptake in skeletal muscle is associated with impaired muscle microvascular exchange capacity (Kf), independently of visceral fat mass. Muscle microvascular function is not improved by 6 months of high-dose statin treatment, despite marked statin-mediated improvements in lipid metabolism and decreased inflammation.
验证以下假设,即肌肉中胰岛素介导的葡萄糖处置减少与肌肉微血管交换能力(Kf)降低有关,且6个月的大剂量他汀类药物治疗可改善中心性肥胖人群的微血管功能。
我们评估了22名女性和17名男性中心性肥胖志愿者的骨骼肌微血管功能、内脏脂肪量、身体活动水平、体能和骨骼肌胰岛素敏感性,这些志愿者的年龄(均值±标准差)为51±9岁。在一项为期6个月的随机、双盲、安慰剂对照试验中,我们测试了阿托伐他汀(每日40毫克)对肌肉微血管功能的影响。
Kf与血糖指标(糖化血红蛋白;r = -0.44,P = 0.006)呈负相关,与胰岛素敏感性(胰岛素刺激的葡萄糖效能即M值与平均胰岛素浓度即I值的比值;r = 0.39,P = 0.02)呈正相关。在回归模型中,糖化血红蛋白、内脏脂肪量和M:I解释了Kf变异的38%(在以Kf为结果的线性回归模型中[R2 = 0.38,P = 0.005])。M:I与Kf相关,且独立于内脏脂肪量(B系数3.13[95%可信区间0.22 - 6.02],P = 0.036)。尽管阿托伐他汀治疗6个月使低密度脂蛋白胆固醇降低了51%(P < 0.001),血浆高敏C反应蛋白降低了75%(P = 0.02),但微血管功能未改变。
骨骼肌中胰岛素介导的葡萄糖摄取减少与肌肉微血管交换能力(Kf)受损有关,且独立于内脏脂肪量。尽管他汀类药物显著改善了脂质代谢并减轻了炎症,但6个月的大剂量他汀治疗并未改善肌肉微血管功能。