Ranucci Marco, Ballotta Andrea, Frigiola Alessandro, Boncilli Alessandra, Brozzi Simonetta, Costa Elena, Mehta Rajendra H
Department of Cardiothoracic-Vascular Anesthesia and Intensive Care, IRCCS Policlinico S.Donato, Milan, Italy.
Eur Heart J. 2009 Apr;30(8):995-1004. doi: 10.1093/eurheartj/ehp015. Epub 2009 Feb 17.
Elevated homocysteinaemia is associated not only with an increased risk for cardiovascular disease but also for increased morbidity and mortality in patients with established coronary artery or cerebrovascular disease. Whether elevated homocysteine further increases the morbidity and mortality in patients undergoing cardiac surgery on cardiopulmonary bypass (CPB) (a prothrombotic state itself) remains less known.
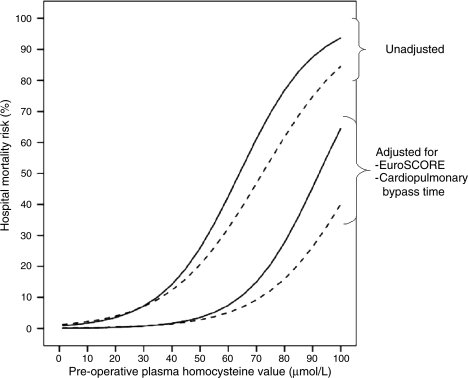
Accordingly, we conducted a prospective observational study with pre-operative measurement of plasma homocysteine levels in 531 consecutive patients undergoing cardiac operations on CPB. The association of pre-operative plasma homocysteine levels with post-operative morbidity and hospital mortality was evaluated. Elevated homocysteine levels (>15 micromol/L) were observed in 209 patients (39.4%), and homocysteinaemia was associated with a higher mortality and perioperative morbidity (major morbidity, low cardiac output, acute renal failure, mesenteric infarction, and thrombo-embolic events). Even after accounting for the differences in baseline clinical features, EuroSCORE, and CPB time, pre-operative homocysteine levels remained independently associated with hospital mortality [odds ratio (OR) 1.06, 95% confidence interval (CI) 1.03-1.11], major morbidity (OR 1.04, 95% CI 1.01-1.07), low cardiac output (OR 1.04, 95% CI 1.02-1.08), mesenteric infarction (OR 1.06, 95% CI 1.01-1.11), and thrombo-embolic events (OR 1.09, 95% CI 1.04-1.13). This association of homocysteine with increased risk of morbidity and mortality was observed particularly in CABG patients.
Elevated pre-operative homocysteine level is independently associated with increased morbidity and mortality, particularly in patients undergoing CABG. Specific post-operative antithrombotic strategies may be advisable in hyperhomocysteinaemic patients.
高同型半胱氨酸血症不仅与心血管疾病风险增加有关,还与已确诊冠状动脉疾病或脑血管疾病患者的发病率和死亡率增加有关。高同型半胱氨酸是否会进一步增加接受体外循环心脏手术(CPB,其本身就是一种血栓形成前状态)患者的发病率和死亡率,目前仍鲜为人知。
因此,我们进行了一项前瞻性观察性研究,对531例连续接受CPB心脏手术的患者术前测量血浆同型半胱氨酸水平。评估术前血浆同型半胱氨酸水平与术后发病率及医院死亡率之间的关联。209例患者(39.4%)观察到同型半胱氨酸水平升高(>15微摩尔/升),高同型半胱氨酸血症与较高的死亡率和围手术期发病率(严重发病率、低心排血量、急性肾衰竭、肠系膜梗死和血栓栓塞事件)相关。即使在考虑了基线临床特征、欧洲心脏手术风险评估系统(EuroSCORE)和CPB时间的差异后,术前同型半胱氨酸水平仍与医院死亡率[比值比(OR)1.06,95%置信区间(CI)1.03 - 1.11]、严重发病率(OR 1.04,95% CI 1.01 - 1.07)、低心排血量(OR 1.04,95% CI 1.02 - 1.08)、肠系膜梗死(OR 1.06,95% CI 1.01 - 1.11)和血栓栓塞事件(OR 1.09,95% CI 1.04 - 1.13)独立相关。同型半胱氨酸与发病率和死亡率风险增加之间的这种关联在冠状动脉搭桥术(CABG)患者中尤为明显。
术前同型半胱氨酸水平升高与发病率和死亡率增加独立相关,尤其是在接受CABG的患者中。对于高同型半胱氨酸血症患者,术后采取特定的抗血栓策略可能是可取的。