Fenaux Pierre, Mufti Ghulam J, Hellstrom-Lindberg Eva, Santini Valeria, Finelli Carlo, Giagounidis Aristoteles, Schoch Robert, Gattermann Norbert, Sanz Guillermo, List Alan, Gore Steven D, Seymour John F, Bennett John M, Byrd John, Backstrom Jay, Zimmerman Linda, McKenzie David, Beach Cl, Silverman Lewis R
Hôpital Avicenne, Université Paris XIII, Bobigny, France.
Lancet Oncol. 2009 Mar;10(3):223-32. doi: 10.1016/S1470-2045(09)70003-8. Epub 2009 Feb 21.
Drug treatments for patients with high-risk myelodysplastic syndromes provide no survival advantage. In this trial, we aimed to assess the effect of azacitidine on overall survival compared with the three commonest conventional care regimens.
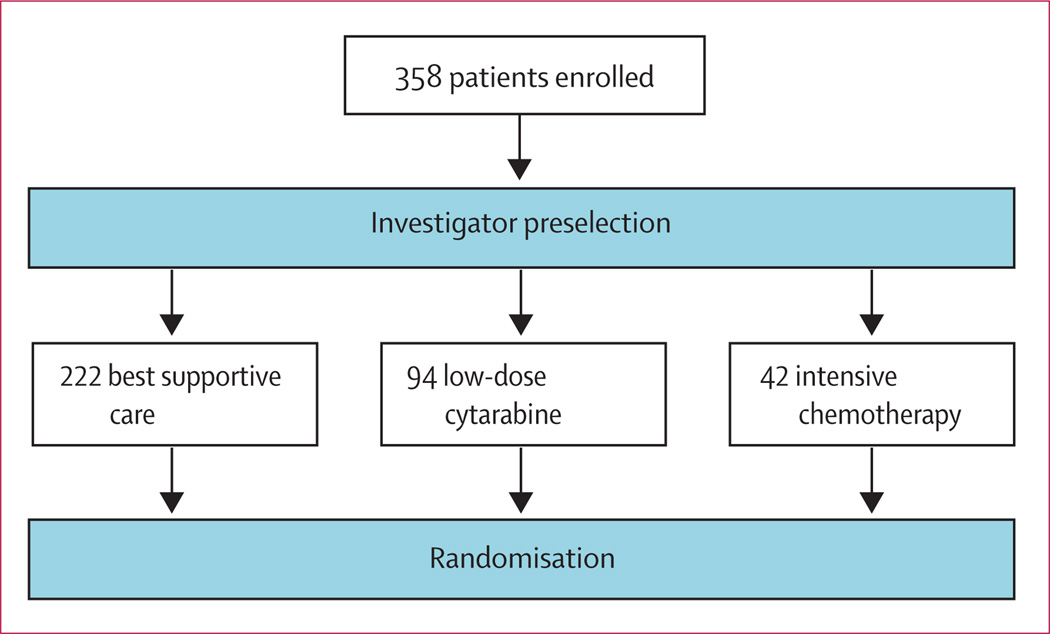
In a phase III, international, multicentre, controlled, parallel-group, open-label trial, patients with higher-risk myelodysplastic syndromes were randomly assigned one-to-one to receive azacitidine (75 mg/m(2) per day for 7 days every 28 days) or conventional care (best supportive care, low-dose cytarabine, or intensive chemotherapy as selected by investigators before randomisation). Patients were stratified by French-American-British and international prognostic scoring system classifications; randomisation was done with a block size of four. The primary endpoint was overall survival. Efficacy analyses were by intention to treat for all patients assigned to receive treatment. This study is registered with ClinicalTrials.gov, number NCT00071799.
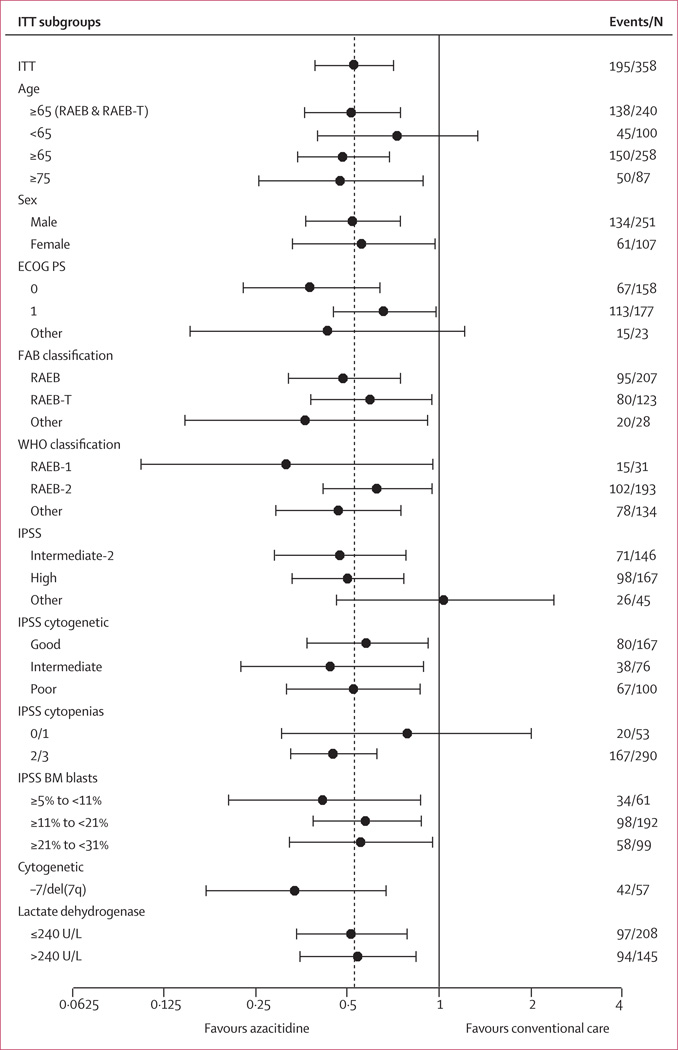
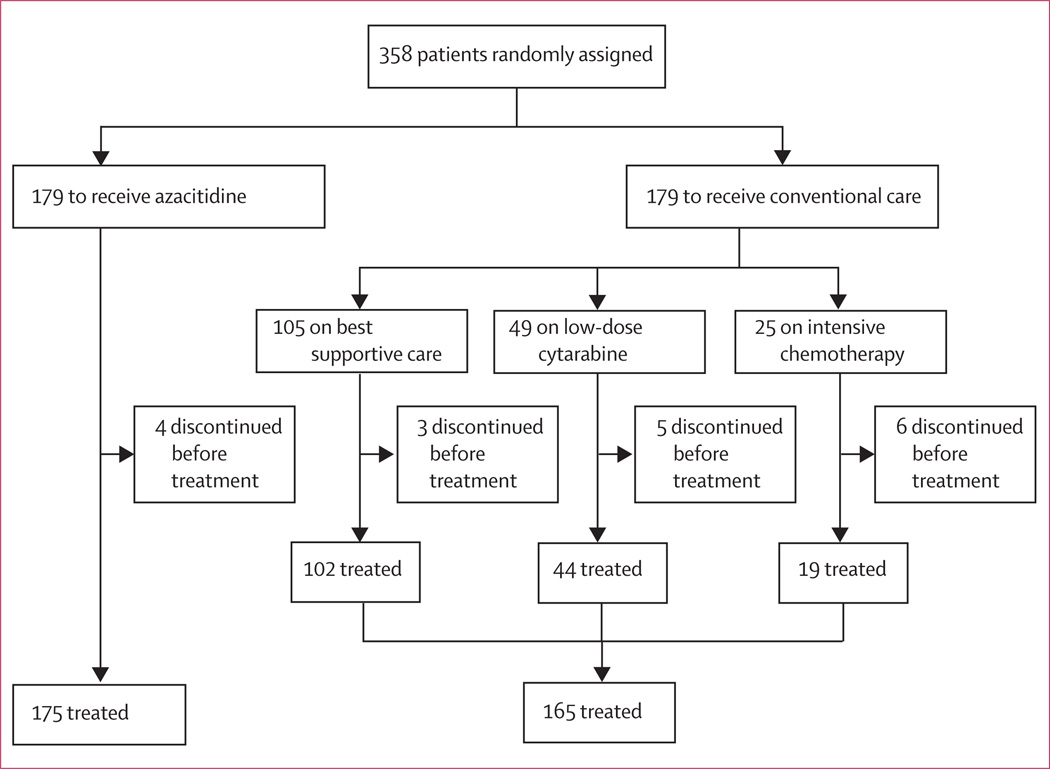
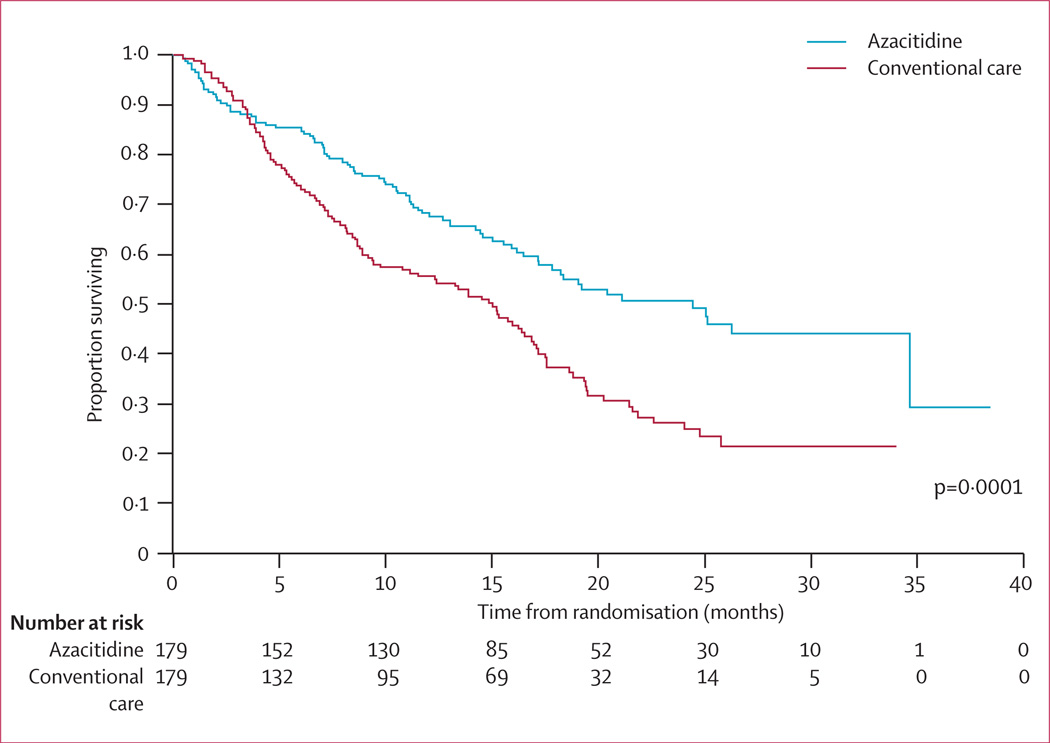
Between Feb 13, 2004, and Aug 7, 2006, 358 patients were randomly assigned to receive azacitidine (n=179) or conventional care regimens (n=179). Four patients in the azacitidine and 14 in the conventional care groups received no study drugs but were included in the intention-to-treat efficacy analysis. After a median follow-up of 21.1 months (IQR 15.1-26.9), median overall survival was 24.5 months (9.9-not reached) for the azacitidine group versus 15.0 months (5.6-24.1) for the conventional care group (hazard ratio 0.58; 95% CI 0.43-0.77; stratified log-rank p=0.0001). At last follow-up, 82 patients in the azacitidine group had died compared with 113 in the conventional care group. At 2 years, on the basis of Kaplan-Meier estimates, 50.8% (95% CI 42.1-58.8) of patients in the azacitidine group were alive compared with 26.2% (18.7-34.3) in the conventional care group (p<0.0001). Peripheral cytopenias were the most common grade 3-4 adverse events for all treatments.
Treatment with azacitidine increases overall survival in patients with higher-risk myelodysplastic syndromes relative to conventional care.
高危骨髓增生异常综合征患者的药物治疗未显示出生存优势。在本试验中,我们旨在评估阿扎胞苷与三种最常用的传统治疗方案相比对总生存期的影响。
在一项III期、国际、多中心、对照、平行组、开放标签试验中,将高危骨髓增生异常综合征患者一对一随机分组,分别接受阿扎胞苷(每28天每天75mg/m²,共7天)或传统治疗(最佳支持治疗、小剂量阿糖胞苷或随机分组前研究者选择的强化化疗)。患者按法国-美国-英国和国际预后评分系统分类进行分层;随机分组采用4的区组大小。主要终点为总生存期。对所有分配接受治疗的患者按意向性治疗进行疗效分析。本研究已在ClinicalTrials.gov注册(编号NCT00071799)。
在2004年2月13日至2006年8月7日期间,358例患者被随机分配接受阿扎胞苷(n = 179)或传统治疗方案(n = 179)。阿扎胞苷组有4例患者和传统治疗组有14例患者未接受研究药物,但被纳入意向性治疗疗效分析。中位随访21.1个月(四分位间距15.1 - 26.9)后,阿扎胞苷组的中位总生存期为24.5个月(9.9 - 未达到),而传统治疗组为15.0个月(5.6 - 24.1)(风险比0.58;95%可信区间0.43 - 0.77;分层对数秩检验p = 0.0001)。在最后一次随访时,阿扎胞苷组有82例患者死亡,而传统治疗组有113例。根据Kaplan-Meier估计,2年时阿扎胞苷组50.8%(95%可信区间42.1 - 58.8)的患者存活,而传统治疗组为26.2%(18.7 - 34.3)(p < 0.0001)。外周血细胞减少是所有治疗中最常见的3 - 4级不良事件。
与传统治疗相比,阿扎胞苷治疗可提高高危骨髓增生异常综合征患者的总生存期。