Parikh Nisha I, Gona Philimon, Larson Martin G, Fox Caroline S, Benjamin Emelia J, Murabito Joanne M, O'Donnell Christopher J, Vasan Ramachandran S, Levy Daniel
National Heart, Lung, and Blood Institute's Framingham Heart Study, Framingham, MA 01702-5803, USA.
Circulation. 2009 Mar 10;119(9):1203-10. doi: 10.1161/CIRCULATIONAHA.108.825364. Epub 2009 Feb 23.
Whereas the prevalence of coronary heart disease risk factors has declined over the past decades in the United States, acute myocardial infarction (AMI) rates have been steady. We hypothesized that this paradox is due partly to the advent of increasingly sensitive biomarkers for AMI diagnosis.
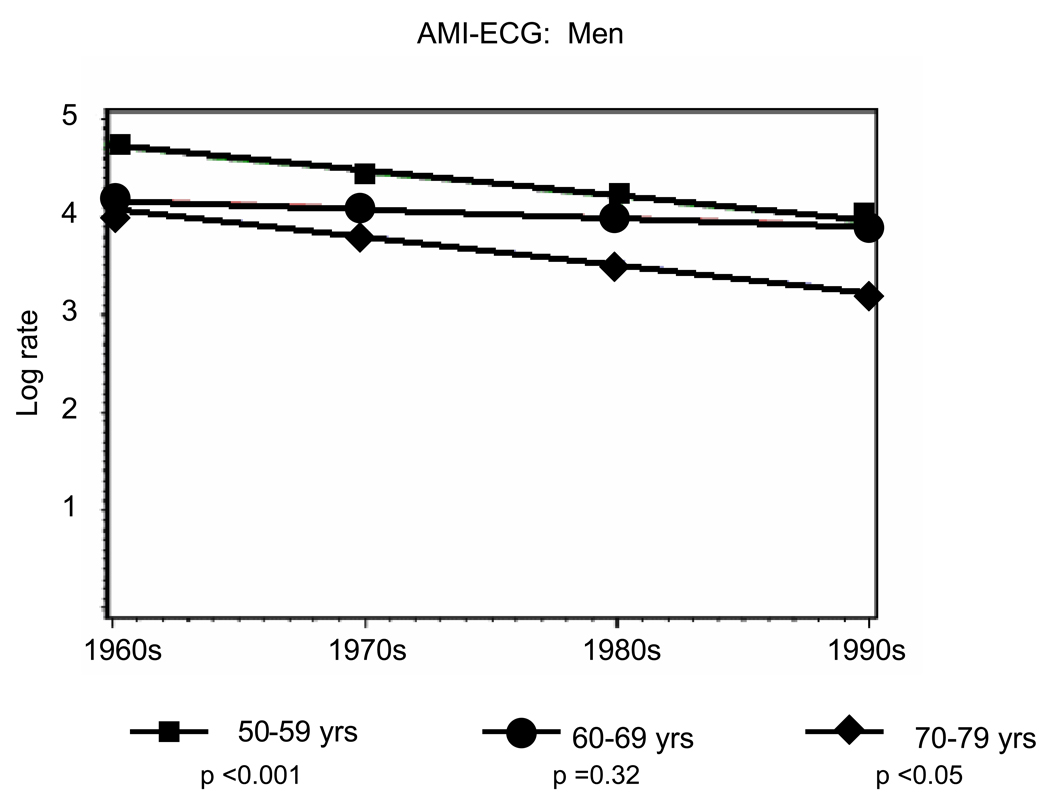
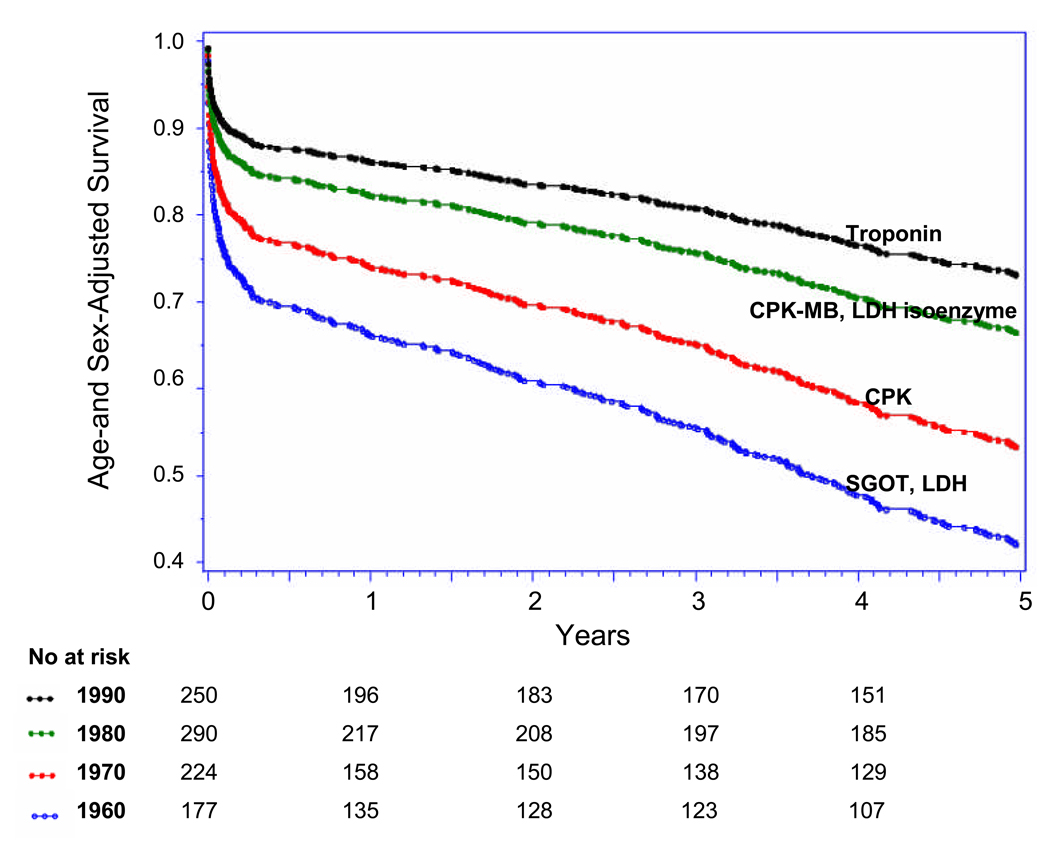
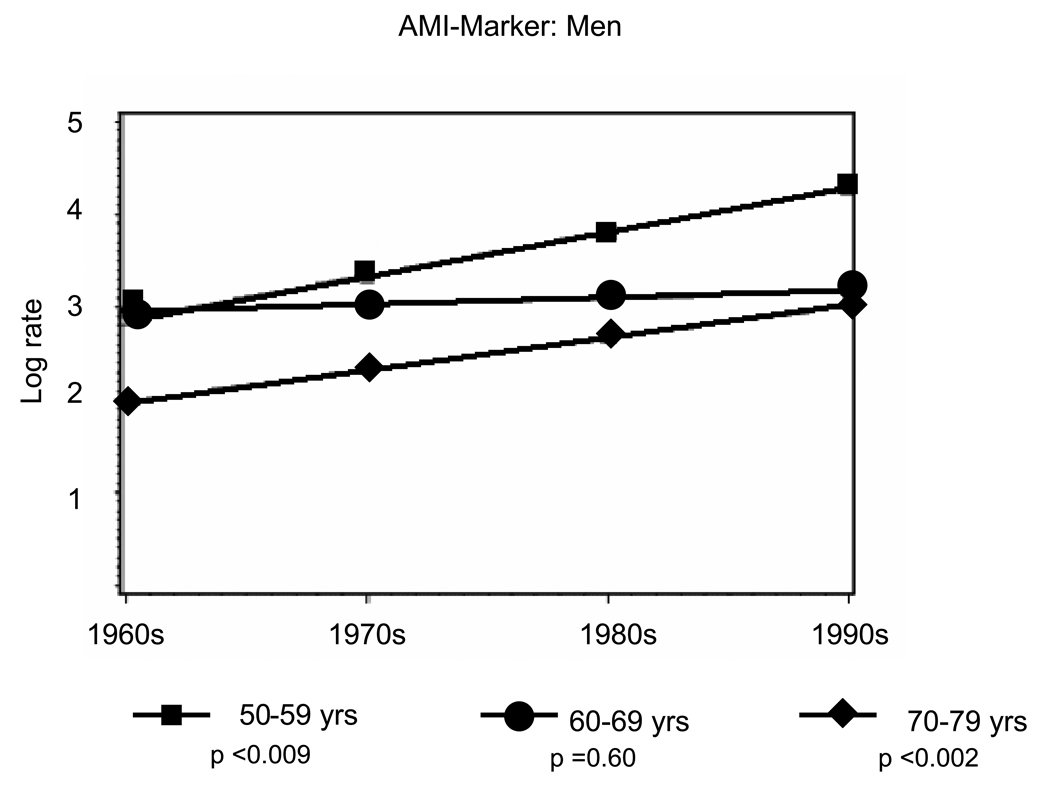
In Framingham Heart Study participants over 4 decades, we compared the incidence and survival rates of initial AMI diagnosis by ECG (AMI-ECG) regardless of biomarkers with those based exclusively on infarction biomarkers (AMI-marker). We used Poisson regression to calculate annual incidence rates of first AMI over 4 decades (1960 to 1969, 1970 to 1979, 1980 to 1989, and 1990 to 1999) and compared rates of AMI-ECG with rates of AMI-marker. Cox proportional-hazards analysis was used to compare AMI case fatality over 4 decades. In 9824 persons (54% women; follow-up, 212 539 person-years; age, 40 to 89 years), 941 AMIs occurred, including 639 AMI-ECG and 302 AMI-marker events. From 1960 to 1999, rates of AMI-ECG declined by approximately 50% and rates of AMI-marker increased approximately 2-fold. Crude 30-day, 1-year, and 5-year case fatality rates in 1960 to 1969 and 1990 to 1999 were 0.20 and 0.14, 0.24 and 0.21, and 0.45 and 0.41, respectively. Age- and sex-adjusted 30-day, 1-year, and 5-year AMI case fatality declined by 60% in 1960 to 1999 (P for trend <0.001), with parallel declines noted after AMI-ECG and AMI-marker.
Over the past 40 years, rates of AMI-ECG have declined by 50%, whereas rates of AMI-marker have doubled. Our findings offer an explanation for the apparently steady national AMI rates in the face of improvements in primary prevention.
尽管在过去几十年中,美国冠心病危险因素的患病率有所下降,但急性心肌梗死(AMI)的发病率一直保持稳定。我们推测,这种矛盾现象部分归因于用于AMI诊断的生物标志物越来越敏感。
在弗雷明汉心脏研究中,我们对40多年来的参与者进行了研究,比较了无论生物标志物如何,通过心电图诊断的首次AMI(AMI-ECG)的发病率和生存率与仅基于梗死生物标志物诊断的AMI(AMI-标志物)的发病率和生存率。我们使用泊松回归计算了40多年(1960年至1969年、1970年至1979年、1980年至1989年和1990年至1999年)首次AMI的年发病率,并比较了AMI-ECG与AMI-标志物的发病率。使用Cox比例风险分析比较了40多年来AMI的病死率。在9824人(54%为女性;随访时间为212539人年;年龄为40至89岁)中,发生了941例AMI,包括639例AMI-ECG事件和302例AMI-标志物事件。从1960年到1999年,AMI-ECG的发病率下降了约50%,而AMI-标志物的发病率增加了约2倍。1960年至1969年和1990年至1999年的30天、1年和5年粗病死率分别为0.20和0.14、0.24和0.21、0.45和0.41。1960年至1999年,年龄和性别调整后的30天、1年和5年AMI病死率下降了60%(趋势P<0.001),AMI-ECG和AMI-标志物后均出现平行下降。
在过去40年中,AMI-ECG的发病率下降了50%,而AMI-标志物的发病率增加了一倍。我们的研究结果为在一级预防有所改善的情况下,全国AMI发病率看似稳定提供了解释。