Nahum Alain, Erhart Annette, Ahounou Daniel, Bonou Désiré, Van Overmeir Chantal, Menten Joris, Akogbeto Martin, Coosemans Marc, Massougbodji Achille, D'Alessandro Umberto
Centre de Recherches Entomologiques de Cotonou, Cotonou, Bénin.
Malar J. 2009 Mar 3;8:37. doi: 10.1186/1475-2875-8-37.
A study carried out in 2003-2005 in Southern Benin showed a day-28 sulphadoxine-pyrimethamine (SP) monotherapy failure rate greater than 40%, while for SP combined with artesunate (SP-AS) the failure rate was 5.3%. Such a large difference could be explained by the relatively short 28-day follow-up period, with a substantial number of recurrent infections possibly occurring after day 28. This paper reports the treatment outcome observed in the same study cohort beyond the initial 28-day follow-up.
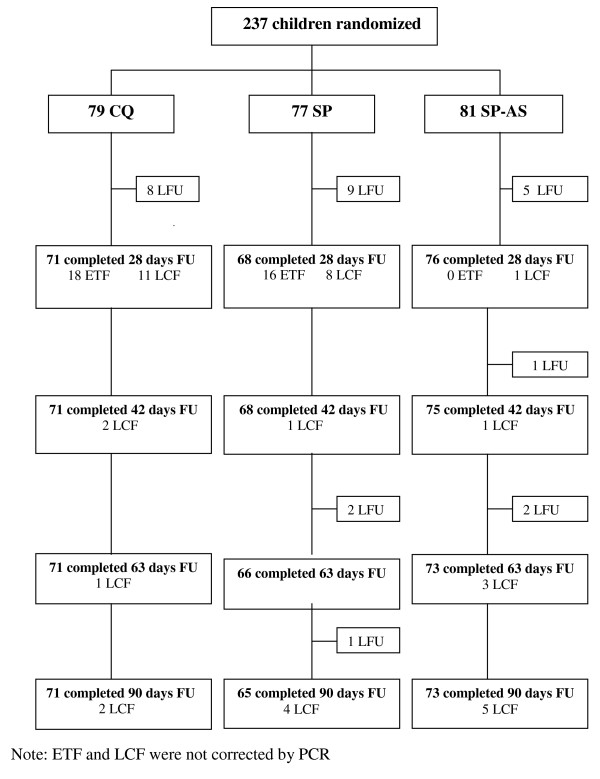
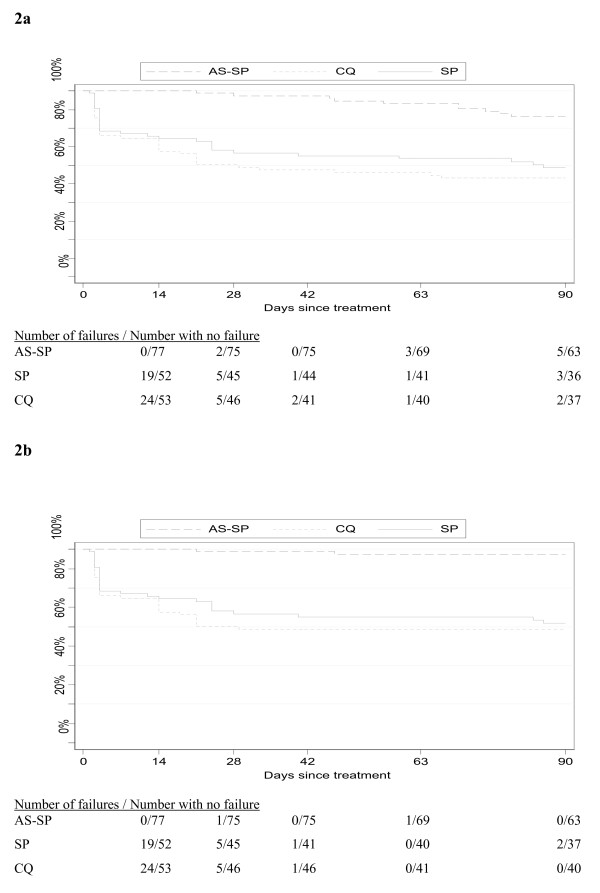
After the 28-day follow-up, children treated with either chloroquine alone (CQ), SP or SP-AS, were visited at home twice a week until day 90 after treatment. A blood sample was collected if the child had fever (axillary temperature > or =37.5 degrees C). Total clinical failure for each treatment group was estimated by combining all the early treatment failures and late clinical failures that occurred over the whole follow-up period, i.e. from day 0 up to day 90. Pre-treatment randomly selected blood samples were genotyped for the dhfr gene (59) and the dhps gene (437 and 540) point mutations related to SP resistance.
The PCR-corrected clinical failure at day 90 was significantly lower in the SP-AS group (SP-AS: 2.7%, SP alone: 38.2%; CQ: 41.1%) (Log-Rank p < 0,001). The most prevalent haplotype was dhfr Arg-59 with the dhps Gly-437 mutant and the dhps 540 wild type (85.5%). The dhps 540 mutation could be found in only three (8.3%) samples.
Combining artesunate to SP dramatically increased the treatment efficacy, even when extending the follow-up to day 90 post-treatment, and despite the high percentage of failures following treatment with SP alone. Such a good performance may be explained by the low prevalence of the dhps 540 mutation, by the rapid parasite clearance with artesunate and by the level of acquired immunity.
2003年至2005年在贝宁南部开展的一项研究显示,磺胺多辛-乙胺嘧啶(SP)单药治疗在第28天的失败率超过40%,而SP与青蒿琥酯联合使用(SP-AS)时失败率为5.3%。如此大的差异可能是由于相对较短的28天随访期,大量复发性感染可能在第28天后发生。本文报告了在同一研究队列中初始28天随访期之后观察到的治疗结果。
在28天随访期之后,对单独使用氯喹(CQ)、SP或SP-AS治疗的儿童,每周两次进行家访,直至治疗后第90天。如果儿童发烧(腋温≥37.5摄氏度)则采集血样。通过合并整个随访期(即从第0天至第90天)内发生的所有早期治疗失败和晚期临床失败来估计每个治疗组的总临床失败情况。对治疗前随机选取的血样进行基因分型,检测与SP耐药相关的二氢叶酸还原酶(dhfr)基因(59位点)以及二氢蝶酸合酶(dhps)基因(437和540位点)的点突变。
在第90天,经PCR校正后的临床失败率在SP-AS组显著更低(SP-AS组:2.7%,单独使用SP组:38.2%;CQ组:4俯涪碘皇鄢郝碉酮冬捆1.1%)(对数秩检验p<0.001)。最常见的单倍型是带有dhps Gly-437突变体和dhps 540野生型的dhfr Arg-59(85.5%)。仅在三个(8.3%)样本中发现了dhps 540突变。
即使将随访期延长至治疗后第90天,且单独使用SP治疗后的失败率很高,但将青蒿琥酯与SP联合使用可显著提高治疗效果。如此良好的治疗效果可能是由于dhps 540突变的低发生率、青蒿琥酯对寄生虫的快速清除作用以及获得性免疫水平。