Kiene J, Schulz Arndt P, Hillbricht S, Jürgens Ch, Paech A
University Hospital Luebeck, Germany.
Eur J Med Res. 2009 Jan 28;14(1):25-9. doi: 10.1186/2047-783x-14-1-25.
The methods for ankle arthrodesis differ significantly, probably a sign that no method is clearly superior to others. In the last ten years there is a clear favour toward internal fixation. We retrospectively evaluate the technique and evaluate the clinical long term results of external fixation in a triangular frame.
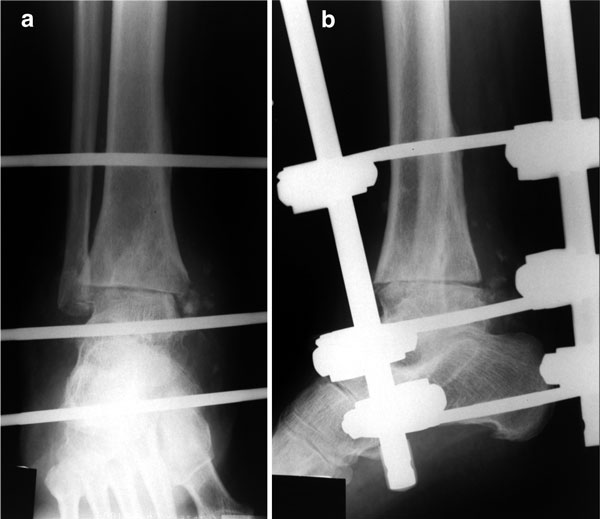
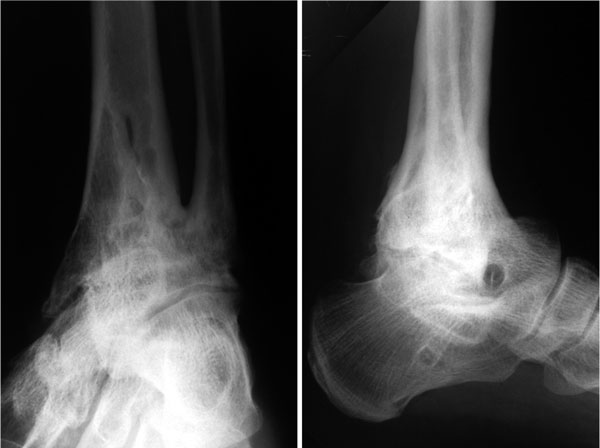
From 1994 to 2001 a consecutive series of 95 patients with end stage arthritis of the ankle joint were treated. Retrospectively the case notes were evaluated regarding trauma history, medical complaints, further injuries and illnesses, walking and pain status and occupational issues and the clinical examination before arthrodesis. Mean age at the index procedure was 45.4 years (18-82), 67 patients were male (70.5%). Via a bilateral approach the malleoli and the joint surfaces were resected. An AO fixator was applied with two Steinmann-nails inserted with approximately 8 cm distance in the distal tibia, one in the neck of the talus and one in the dorsal calcaneus. The fixator was removed after approximately 12 weeks. Follow up examination at mean 4.4 years included a standardised questionnaire and a clinical examination including the criteria of the AOFAS-Score and radiographs.
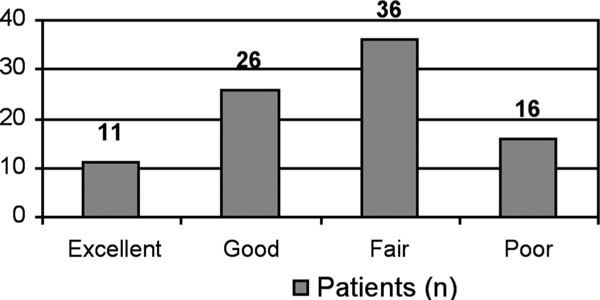
Due to different complications, 8 (8.9%) further surgical procedures were necessary including 1 below knee amputation. In 4 patients a non-union of the ankle arthrodesis developed (4.5%). The mean AOFAS score improved from 20.8 to 69.3 points.
Non-union rates and clinical results of arthrodesis by triangular external fixation of the ankle joint do not differ to internal fixation methods. The complication rate and the reduced patient comfort reserve this method mainly for infected arthritis and complicated soft tissue situations.
踝关节融合术的方法差异很大,这可能表明没有一种方法明显优于其他方法。在过去十年中,明显倾向于采用内固定。我们回顾性评估了一种三角架外固定技术,并评估了其临床长期效果。
1994年至2001年,连续治疗了95例踝关节终末期关节炎患者。回顾性评估病历,包括创伤史、医疗主诉、其他损伤和疾病、行走和疼痛状况、职业问题以及关节融合术前的临床检查。初次手术时的平均年龄为45.4岁(18 - 82岁),67例为男性(70.5%)。通过双侧入路切除内外踝和关节面。应用AO固定器,在胫骨远端插入两根斯氏针,相距约8厘米,一根插入距骨颈,一根插入跟骨背侧。约12周后取出固定器。平均4.4年的随访检查包括一份标准化问卷和一次临床检查,包括AOFAS评分标准及X线片。
由于不同并发症,需要进行8例(8.9%)进一步手术,其中包括1例膝下截肢。4例患者发生踝关节融合术不愈合(4.5%)。AOFAS评分平均从20.8分提高到69.3分。
踝关节三角外固定融合术的不愈合率和临床结果与内固定方法无差异。并发症发生率以及患者舒适度降低使得这种方法主要用于感染性关节炎和复杂软组织情况。