Kerachian Mohammad Amin, Séguin Chantal, Harvey Edward J
Department of Human Genetics, McGill University Health Center, Montreal, Canada.
J Steroid Biochem Mol Biol. 2009 Apr;114(3-5):121-8. doi: 10.1016/j.jsbmb.2009.02.007. Epub 2009 Feb 21.
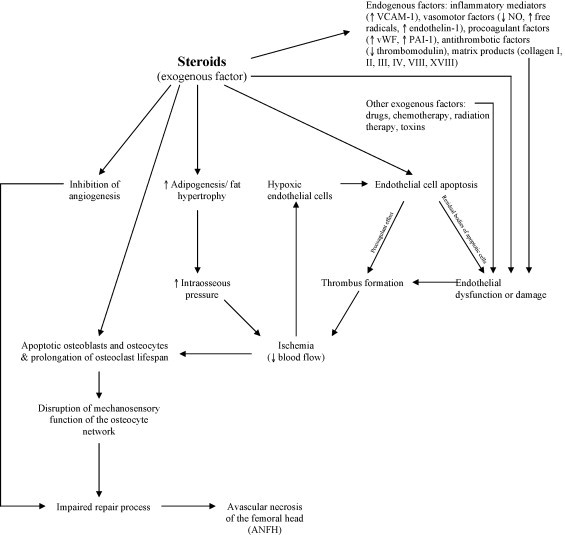
Glucocorticoid (GC) usage is the most common non-traumatic cause of osteonecrosis of the femoral head (ON). Despite the strong association of GC with ON, the underlying mechanisms have been unclear. Investigators have proposed both direct and indirect effects of GC on cells. Indirect and direct mechanisms remain intimately related and often result in positive feedback loops to potentiate the disease processes. However, the direct effects, in particular apoptosis, have recently been shown to be increasingly important. Suppression of osteoblast and osteoclast precursor production, increased apoptosis of osteoblasts and osteocytes, prolongation of the lifespan of osteoclasts and apoptosis of endothelial cells (EC) are all direct effects of GC usage. Elevated blood pressure through several pathways may raise the risk of clot formation. High-dose GC also decreases tissue plasminogen activator activity (t-PA) and increases plasma plasminogen activator inhibitor-1 (PAI-1) antigen levels increasing the procoagulant potential of GC. Inhibited angiogenesis, altered bone repair and nitric oxide metabolism can also result. Also, GC treatment modulates other vasoactive mediators such as endothelin-1, noradrenalin and bradykinin. Thus, GCs act as a regulator of local blood flow by modulating vascular responsiveness to vasoactive substances. Vasoconstriction induced in intraosseous femoral head arteries causes femoral head ischemia. GCs also cause ischemia through increased intraosseous pressure, which subsequently decreases the blood flow to the femoral head by apoptosis of ECs as well as elevating the level of adipogenesis and fat hypertrophy in the bone marrow. It is difficult to predict which patients receiving a specific dose of GC will develop ON, indicating individual differences in steroid sensitivity and the potential of additional mechanisms. The textbook model of ON is a multiple hit theory in which, with a greater number of risk factors, the risk of ON increases. While more effort is needed to better comprehend the role of GC in ON, newer data on GC action upon the endothelial cell and the regional endothelial bed dysfunction theory sheds new light on particular GC mechanisms. Better understanding of GC pathomechanisms can lead to better treatment options.
糖皮质激素(GC)的使用是股骨头坏死(ON)最常见的非创伤性病因。尽管GC与ON之间存在密切关联,但其潜在机制尚不清楚。研究人员提出了GC对细胞的直接和间接作用。间接和直接机制密切相关,常常导致正反馈循环,从而加剧疾病进程。然而,最近研究表明,直接作用,尤其是细胞凋亡,变得越来越重要。抑制成骨细胞和破骨细胞前体的产生、增加成骨细胞和骨细胞的凋亡、延长破骨细胞的寿命以及内皮细胞(EC)的凋亡都是GC使用的直接作用。通过多种途径升高血压可能会增加血栓形成的风险。高剂量GC还会降低组织纤溶酶原激活物活性(t-PA),并增加血浆纤溶酶原激活物抑制剂-1(PAI-1)抗原水平,从而增加GC的促凝潜力。此外,还可能导致血管生成受抑制、骨修复改变以及一氧化氮代谢异常。而且,GC治疗会调节其他血管活性介质,如内皮素-1、去甲肾上腺素和缓激肽。因此,GC通过调节血管对血管活性物质的反应性来充当局部血流的调节剂。股骨头骨内动脉诱导的血管收缩会导致股骨头缺血。GC还会通过增加骨内压导致缺血,随后通过EC凋亡减少股骨头的血流,并提高骨髓中脂肪生成和脂肪肥大的水平。很难预测哪些接受特定剂量GC治疗的患者会发生ON,这表明个体对类固醇的敏感性存在差异,并且可能存在其他机制。ON的经典模型是多重打击理论,即风险因素越多,发生ON的风险就越高。虽然需要更多努力来更好地理解GC在ON中的作用,但关于GC对内皮细胞作用的最新数据以及局部内皮床功能障碍理论为特定的GC机制提供了新的线索。更好地理解GC的发病机制可以带来更好的治疗选择。