Uusitupa Matti, Peltonen Markku, Lindström Jaana, Aunola Sirkka, Ilanne-Parikka Pirjo, Keinänen-Kiukaanniemi Sirkka, Valle Timo T, Eriksson Johan G, Tuomilehto Jaakko
School of Public Health and Clinical Nutrition, Food and Health Research Centre, University of Kuopio, Kuopio, Finland.
PLoS One. 2009 May 21;4(5):e5656. doi: 10.1371/journal.pone.0005656.
The Finnish Diabetes Prevention Study (DPS) was a randomized controlled trial, which showed that it is possible to prevent type 2 diabetes by lifestyle changes. The aim of the present study was to examine whether the lifestyle intervention had an effect on the ten-year mortality and cardiovascular morbidity in the DPS participants originally randomized either into an intervention or control group. Furthermore, we compared these results with a population-based cohort comprising individuals of varying glucose tolerance states.
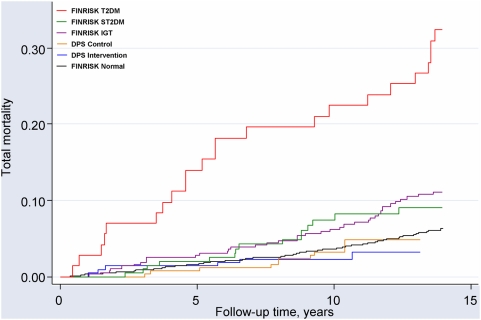
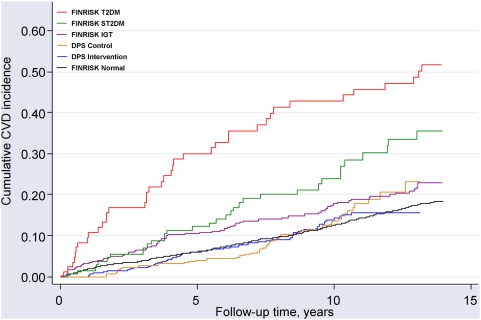
Middle-aged, overweight people with IGT (n = 522) were randomized into intensive intervention (including physical activity, weight reduction and dietary counseling), or control "mini-intervention" group. Median length of the intervention period was 4 years and the mean follow-up was 10.6 years. The population-based reference study cohort included 1881 individuals (1570 with normal glucose tolerance, 183 with IGT, 59 with screen-detected type 2 diabetes, 69 with previously known type 2 diabetes) with the mean follow-up of 13.8 years. Mortality and cardiovascular morbidity data were collected from the national Hospital Discharge Register and Causes of Death Register. Among the DPS participants who consented for register linkage (n = 505), total mortality (2.2 vs. 3.8 per 1000 person years, hazard ratio HR = 0.57, 95% CI 0.21-1.58) and cardiovascular morbidity (22.9 vs. 22.0 per 1000 person years, HR = 1.04, 95% CI 0.72-1.51) did not differ significantly between the intervention and control groups. Compared with the population-based cohort with impaired glucose tolerance, adjusted HRs were 0.21 (95% CI 0.09-0.52) and 0.39 (95% CI 0.20-0.79) for total mortality, and 0.89 (95% CI 0.62-1.27) and 0.87 (0.60-1.27) for cardiovascular morbidity in the intervention and control groups of the DPS, respectively. The risk of death in DPS combined cohort was markedly lower than in FINRISK IGT cohort (adjusted HR 0.30, 95% CI 0.17-0.54), but there was no significant difference in the risk of CVD (adjusted HR 0.88, 95% CI 0.64-1.21).
Lifestyle intervention among persons with IGT did not decrease cardiovascular morbidity during the first 10 years of follow-up. However, the statistical power may not be sufficient to detect small differences between the intervention and control groups. Low total mortality among participants of the DPS compared with individuals with IGT in the general population could be ascribed to a lower cardiovascular risk profile at baseline and regular follow-up.
ClinicalTrials.gov NCT00518167.
芬兰糖尿病预防研究(DPS)是一项随机对照试验,该试验表明通过生活方式改变可以预防2型糖尿病。本研究的目的是检验生活方式干预对最初被随机分配到干预组或对照组的DPS参与者的十年死亡率和心血管疾病发病率是否有影响。此外,我们将这些结果与一个基于人群的队列进行了比较,该队列包括不同糖耐量状态的个体。
522名中年超重的糖耐量受损(IGT)者被随机分为强化干预组(包括体育活动、减重和饮食咨询)或对照“小干预”组。干预期的中位数为4年,平均随访时间为10.6年。基于人群的参考研究队列包括1881名个体(1570名糖耐量正常者、183名IGT者、59名筛查发现的2型糖尿病患者、69名既往已知的2型糖尿病患者),平均随访时间为13.8年。死亡率和心血管疾病发病率数据从国家医院出院登记册和死亡原因登记册收集。在同意进行登记链接的DPS参与者中(n = 505),干预组和对照组的总死亡率(每1000人年分别为2.2和3.8,风险比HR = 0.57,95%置信区间0.21 - 1.58)和心血管疾病发病率(每1000人年分别为22.9和22.0,HR = 1.04,95%置信区间0.72 - 1.51)没有显著差异。与糖耐量受损的基于人群的队列相比,DPS干预组和对照组的总死亡率调整后HR分别为0.21(95%置信区间0.09 - 0.52)和0.39(95%置信区间0.20 - 0.79),心血管疾病发病率调整后HR分别为0.89(95%置信区间0.62 - 1.27)和0.87(0.60 - 1.27)。DPS合并队列的死亡风险明显低于FINRISK IGT队列(调整后HR 0.30,95%置信区间0.17 - 0.54),但心血管疾病风险没有显著差异(调整后HR 0.88,95%置信区间0.64 - 1.21)。
IGT者的生活方式干预在随访的前10年中并未降低心血管疾病发病率。然而,统计效能可能不足以检测干预组和对照组之间的微小差异。与一般人群中的IGT个体相比,DPS参与者的总死亡率较低可能归因于基线和定期随访时较低的心血管疾病风险状况。
ClinicalTrials.gov NCT00518167。