Djulbegovic Benjamin, Trikalinos Thomas A, Roback John, Chen Ren, Guyatt Gordon
Center for Evidence-based Medicine and Health Outcome Research, Clinical Translational Science Institute, Florida, USA.
BMC Health Serv Res. 2009 Jul 21;9:120. doi: 10.1186/1472-6963-9-120.
Evidence is necessary but not sufficient for decision-making, such as making recommendations by clinical practice guideline panels. However, the fundamental premise of evidence-based medicine (EBM) rests on the assumed link between the quality of evidence and "truth" and/or correctness in making guideline recommendations. If this assumption is accurate, then the quality of evidence ought to play a key role in making guideline recommendations. Surprisingly, and despite the widespread penetration of EBM in health care, there has been no empirical research to date investigating the impact of quality of evidence on the strength of recommendations made by guidelines panels.
The American Association of Blood Banking (AABB) has recently convened a 12 member panel to develop clinical practice guidelines (CPG) for the use of fresh-frozen plasma (FFP) for 6 different clinical indications. The panel was instructed that 4 factors should play a role in making recommendation: quality of evidence, uncertainty about the balance between desirable (benefits) and undesirable effects (harms), uncertainty or variability in values and preferences, and uncertainty about whether the intervention represents a wise use of resources (costs). Each member of the panel was asked to make his/her final judgments on the strength of recommendation and the overall quality of the body of evidence. "Voting" was anonymous and was based on the use of GRADE (Grading quality of evidence and strength of recommendations) system, which clearly distinguishes between quality of evidence and strength of recommendations.
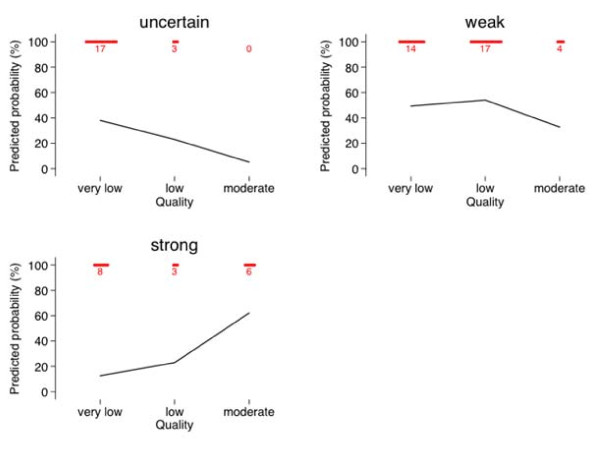
Despite the fact that many factors play role in formulating CPG recommendations, we show that when the quality of evidence is higher, the probability of making a strong recommendation for or against an intervention dramatically increases. Probability of making strong recommendation was 62% when evidence is "moderate", while it was only 23% and 13% when evidence was "low" or "very low", respectively.
We report the first empirical evaluation of the relationship between quality of evidence pertinent to a clinical question and strength of the corresponding guideline recommendations. Understanding the relationship between quality of evidence and probability of making (strong) recommendation has profound implications for the science of quality measurement in health care.
证据对于决策而言是必要的,但并不充分,比如临床实践指南制定小组给出的推荐建议。然而,循证医学(EBM)的基本前提基于证据质量与“真相”以及/或者指南推荐正确性之间的假定联系。如果这一假设准确无误,那么证据质量理应在做出指南推荐时发挥关键作用。令人惊讶的是,尽管循证医学在医疗保健领域已广泛普及,但迄今为止尚无实证研究调查证据质量对指南制定小组所做推荐强度的影响。
美国血库协会(AABB)最近召集了一个由12名成员组成的小组,为新鲜冰冻血浆(FFP)在6种不同临床指征下的使用制定临床实践指南(CPG)。该小组接到指示,在做出推荐时应考虑4个因素:证据质量、有利(益处)与不利影响(危害)之间平衡的不确定性、价值观和偏好的不确定性或变异性,以及干预措施是否合理利用资源(成本)的不确定性。要求小组的每位成员就推荐强度和证据总体质量做出最终判断。“投票”是匿名的,且基于使用GRADE(证据质量分级与推荐强度分级)系统,该系统能清晰区分证据质量和推荐强度。
尽管有许多因素在制定CPG推荐时发挥作用,但我们发现,当证据质量较高时,对干预措施做出强烈支持或反对推荐的可能性会大幅增加。当证据为“中等”时,做出强烈推荐的概率为62%,而当证据为“低”或“极低”时,这一概率分别仅为23%和13%。
我们报告了对与临床问题相关的证据质量和相应指南推荐强度之间关系进行的首次实证评估。理解证据质量与做出(强烈)推荐概率之间的关系,对医疗保健质量测量科学具有深远意义。