Navarro-Sarabia Federico, Ruiz-Montesinos Dolores, Hernandez Blanca, Navarro-Compán Victoria, Marsal Sara, Barcelo Mireia, Perez-Pampín Eva, Gómez-Reino Juan J
Rheumatology Service, Hospital Universitario Virgen Macarena, Sevilla, Spain.
BMC Musculoskelet Disord. 2009 Jul 23;10:91. doi: 10.1186/1471-2474-10-91.
No definitive data are available regarding the value of switching to an alternative TNF antagonist in rheumatoid arthritis patients who fail to respond to the first one. The aim of this study was to evaluate treatment response in a clinical setting based on HAQ improvement and EULAR response criteria in RA patients who were switched to a second or a third TNF antagonist due to failure with the first one.
This was an observational, prospective study of a cohort of 417 RA patients treated with TNF antagonists in three university hospitals in Spain between January 1999 and December 2005. A database was created at the participating centres, with well-defined operational instructions. The main outcome variables were analyzed using parametric or non-parametric tests depending on the level of measurement and distribution of each variable.
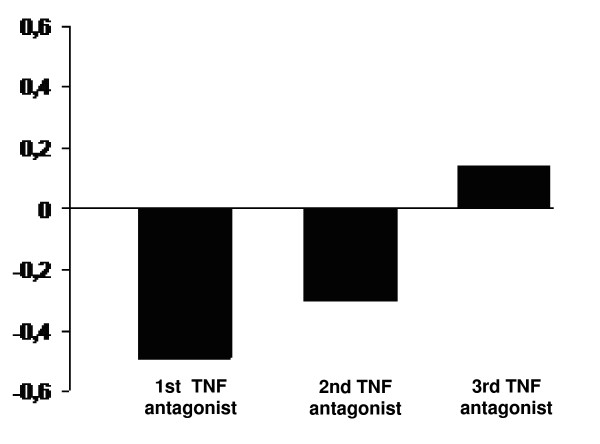
Mean (+/- SD) DAS-28 on starting the first, second and third TNF antagonist was 5.9 (+/- 2.0), 5.1 (+/- 1.5) and 6.1 (+/- 1.1). At the end of follow-up, it decreased to 3.3 (+/- 1.6; Delta = -2.6; p > 0.0001), 4.2 (+/- 1.5; Delta = -1.1; p = 0.0001) and 5.4 (+/- 1.7; Delta = -0.7; p = 0.06). For the first TNF antagonist, DAS-28-based EULAR response level was good in 42% and moderate in 33% of patients. The second TNF antagonist yielded a good response in 20% and no response in 53% of patients, while the third one yielded a good response in 28% and no response in 72%. Mean baseline HAQ on starting the first, second and third TNF antagonist was 1.61, 1.52 and 1.87, respectively. At the end of follow-up, it decreased to 1.12 (Delta = -0.49; p < 0.0001), 1.31 (Delta = -0.21, p = 0.004) and 1.75 (Delta = -0.12; p = 0.1), respectively. Sixty four percent of patients had a clinically important improvement in HAQ (defined as > or = -0.22) with the first TNF antagonist and 46% with the second.
A clinically significant effect size was seen in less than half of RA patients cycling to a second TNF antagonist.
对于类风湿关节炎患者在对第一种肿瘤坏死因子(TNF)拮抗剂治疗无反应时换用另一种TNF拮抗剂的价值,尚无确切数据。本研究的目的是基于健康评估问卷(HAQ)改善情况和欧洲抗风湿病联盟(EULAR)反应标准,在临床环境中评估因对第一种TNF拮抗剂治疗失败而换用第二种或第三种TNF拮抗剂的类风湿关节炎患者的治疗反应。
这是一项对1999年1月至2005年12月期间在西班牙三家大学医院接受TNF拮抗剂治疗的417例类风湿关节炎患者队列进行的观察性前瞻性研究。在参与中心创建了一个数据库,并制定了明确的操作说明。根据每个变量的测量水平和分布情况,使用参数检验或非参数检验分析主要结局变量。
开始使用第一种、第二种和第三种TNF拮抗剂时,平均(±标准差)疾病活动度评分(DAS-28)分别为5.9(±2.0)、5.1(±1.5)和6.1(±1.1)。随访结束时,DAS-28分别降至3.3(±1.6;变化量=-2.6;p>0.0001)、4.2(±1.5;变化量=-1.1;p=0.0001)和5.4(±1.7;变化量=-0.7;p=0.06)。对于第一种TNF拮抗剂,基于DAS-28的EULAR反应水平在42%的患者中为良好,在33%的患者中为中等。第二种TNF拮抗剂在20%的患者中产生良好反应,在53%的患者中无反应,而第三种TNF拮抗剂在28%的患者中产生良好反应,在72%的患者中无反应。开始使用第一种、第二种和第三种TNF拮抗剂时,平均基线HAQ分别为1.61、1.52和1.87。随访结束时,HAQ分别降至1.12(变化量=-0.49;p<0.0001)、1.31(变化量=-0.21,p=0.004)和1.75(变化量=-0.12;p=0.1)。64%的患者使用第一种TNF拮抗剂时HAQ有临床意义的改善(定义为≥-0.22),使用第二种TNF拮抗剂时这一比例为46%。
在不到一半换用第二种TNF拮抗剂的类风湿关节炎患者中观察到具有临床意义的效应量。