Dam Erik B, Loog Marco, Christiansen Claus, Byrjalsen Inger, Folkesson Jenny, Nielsen Mads, Qazi Arish A, Pettersen Paola C, Garnero Patrick, Karsdal Morten A
Nordic Bioscience, Herlev Hovedgade 207, Herlev, Denmark.
Arthritis Res Ther. 2009;11(4):R115. doi: 10.1186/ar2774. Epub 2009 Jul 24.
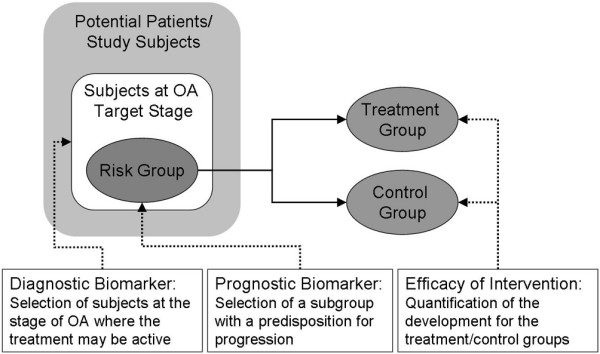
At present, no disease-modifying osteoarthritis drugs (DMOADS) are approved by the FDA (US Food and Drug Administration); possibly partly due to inadequate trial design since efficacy demonstration requires disease progression in the placebo group. We investigated whether combinations of biochemical and magnetic resonance imaging (MRI)-based markers provided effective diagnostic and prognostic tools for identifying subjects with high risk of progression. Specifically, we investigated aggregate cartilage longevity markers combining markers of breakdown, quantity, and quality.
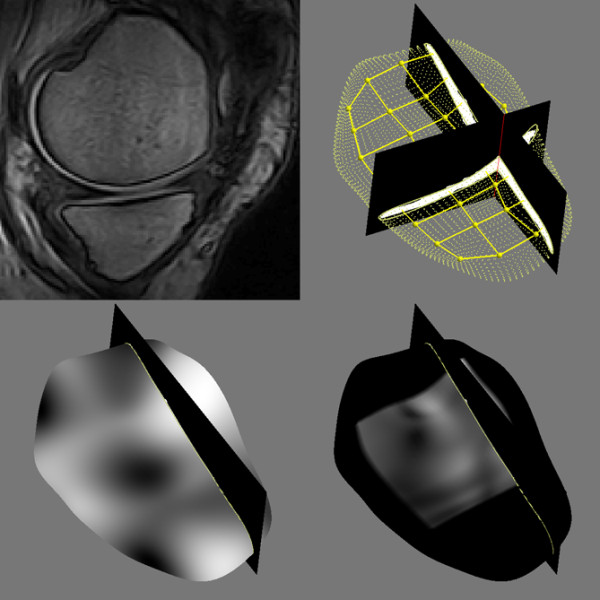
The study included healthy individuals and subjects with radiographic osteoarthritis. In total, 159 subjects (48% female, age 56.0 +/- 15.9 years, body mass index 26.1 +/- 4.2 kg/m2) were recruited. At baseline and after 21 months, biochemical (urinary collagen type II C-telopeptide fragment, CTX-II) and MRI-based markers were quantified. MRI markers included cartilage volume, thickness, area, roughness, homogeneity, and curvature in the medial tibio-femoral compartment. Joint space width was measured from radiographs and at 21 months to assess progression of joint damage.
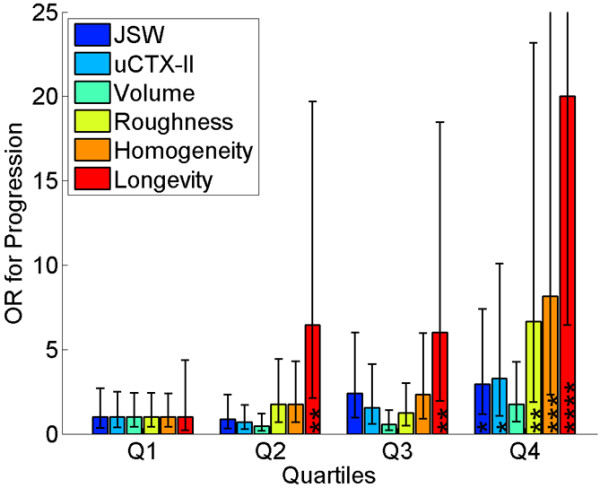
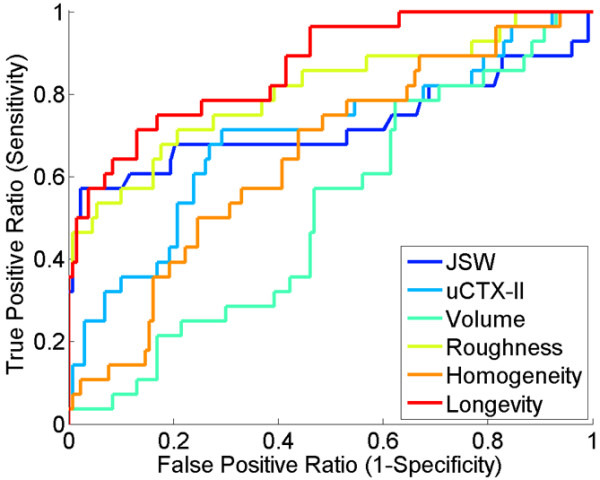
Cartilage roughness had the highest diagnostic accuracy quantified as the area under the receiver-operator characteristics curve (AUC) of 0.80 (95% confidence interval: 0.69 to 0.91) among the individual markers (higher than all others, P < 0.05) to distinguish subjects with radiographic osteoarthritis from healthy controls. Diagnostically, cartilage longevity scored AUC 0.84 (0.77 to 0.92, higher than roughness: P = 0.03). For prediction of longitudinal radiographic progression based on baseline marker values, the individual prognostic marker with highest AUC was homogeneity at 0.71 (0.56 to 0.81). Prognostically, cartilage longevity scored AUC 0.77 (0.62 to 0.90, borderline higher than homogeneity: P = 0.12). When comparing patients in the highest quartile for the longevity score to lowest quartile, the odds ratio of progression was 20.0 (95% confidence interval: 6.4 to 62.1).
Combination of biochemical and MRI-based biomarkers improved diagnosis and prognosis of knee osteoarthritis and may be useful to select high-risk patients for inclusion in DMOAD clinical trials.
目前,美国食品药品监督管理局(FDA)尚未批准任何改变病情的骨关节炎药物(DMOADS);这可能部分归因于试验设计不完善,因为疗效证明需要安慰剂组出现疾病进展。我们研究了基于生化指标和磁共振成像(MRI)的标志物组合是否能为识别疾病进展高危受试者提供有效的诊断和预后工具。具体而言,我们研究了综合软骨寿命标志物,该标志物结合了软骨破坏、数量和质量的标志物。
该研究纳入了健康个体和影像学诊断为骨关节炎的受试者。总共招募了159名受试者(48%为女性,年龄56.0±15.9岁,体重指数26.1±4.2kg/m²)。在基线期和21个月后,对生化指标(尿II型胶原C末端肽片段,CTX-II)和基于MRI的标志物进行定量分析。MRI标志物包括内侧胫股关节软骨体积、厚度、面积、粗糙度、同质性和曲率。通过X线片测量关节间隙宽度,并在21个月时评估关节损伤的进展情况。
在区分影像学诊断为骨关节炎的受试者与健康对照的个体标志物中,软骨粗糙度的诊断准确性最高,其受试者工作特征曲线下面积(AUC)为0.80(95%置信区间:0.69至0.91)(高于所有其他标志物,P<0.05)。在诊断方面,软骨寿命评分的AUC为0.84(0.77至0.92,高于粗糙度:P = 0.03)。基于基线标志物值预测纵向影像学进展时,AUC最高的个体预后标志物是同质性,为0.71(0.56至0.81)。在预后方面,软骨寿命评分的AUC为0.77(0.62至0.90,略高于同质性:P = 0.12)。将寿命评分最高四分位数的患者与最低四分位数的患者进行比较时,进展的优势比为20.0(95%置信区间:6.4至62.1)。
基于生化指标和MRI的生物标志物组合改善了膝关节骨关节炎的诊断和预后,可能有助于选择高危患者纳入DMOAD临床试验。