Castle Philip E, Rodríguez Ana Cecilia, Burk Robert D, Herrero Rolando, Wacholder Sholom, Alfaro Mario, Morales Jorge, Guillen Diego, Sherman Mark E, Solomon Diane, Schiffman Mark
Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, DHHS, Bethesda, MD 20892, USA.
BMJ. 2009 Jul 28;339:b2569. doi: 10.1136/bmj.b2569.
To evaluate the cumulative incidence of cervical intraepithelial neoplasia II or worse (grade II+) or cervical intraepithelial neoplasia grade III+ after short term persistence of prevalently detected carcinogenic human papillomavirus (HPV).
Population based cohort study.
Guanacaste, Costa Rica.
2282 sexually active women actively followed after enrolment.
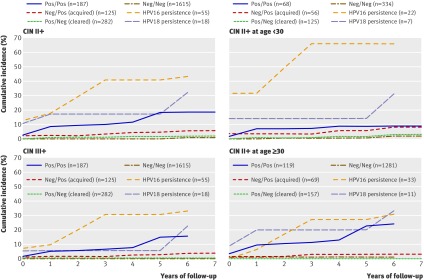
Primary end points: three year and five year cumulative incidence of histologically confirmed cervical intraepithelial neoplasia grade II+ (n=70). Cervical specimens collected at each visit tested for more than 40 HPV genotypes. HPV 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 73, and 82 were considered the primary carcinogenic genotypes.
Women who tested positive for a carcinogenic HPV at enrolment and after about one year (9-21 months) (positive/positive) had a three year cumulative incidence of cervical intraepithelial neoplasia grade II+ of 17.0% (95% confidence interval 12.1% to 22.0%). Those who tested negative/positive (3.4%, 0.1% to 6.8%), positive/negative (1.2%, -0.2% to 2.5%), and negative/negative (0.5%, 0.1% to 0.9%) were at a significantly lower risk. There was little difference in the cumulative incidence of cervical intraepithelial neoplasia grade II+ between testing positive twice for any carcinogenic HPV genotype (same genotype or different genotypes) v testing positive twice for the same carcinogenic genotype (17.0% v 21.3%, respectively). Short term persistence of HPV 16 strongly predicted cervical intraepithelial neoplasia grade II+, with a three year cumulative incidence of 40.8% (26.4% to 55.1%). Similar patterns were observed for the five year cumulative incidence of grade II+ and for three year and five year cumulative incidence of grade III+.
Short term persistence of a prevalently detected carcinogenic HPV infection, especially HPV 16, strongly predicts a subsequent diagnosis of cervical intraepithelial neoplasia II+ over the next few years.
评估普遍检测到的致癌性人乳头瘤病毒(HPV)短期持续存在后,宫颈上皮内瘤变II级或更严重病变(II+级)或宫颈上皮内瘤变III+级的累积发病率。
基于人群的队列研究。
哥斯达黎加瓜纳卡斯特。
2282名性活跃女性,入组后积极随访。
主要终点:组织学确诊的宫颈上皮内瘤变II+级(n = 70)的三年和五年累积发病率。每次访视时收集的宫颈标本检测40多种HPV基因型。HPV 16、18、26、31、33、35、39、45、51、52、56、58、59、66、68、73和82被视为主要致癌基因型。
入组时和大约一年后(9 - 21个月)致癌性HPV检测呈阳性(阳性/阳性)的女性,宫颈上皮内瘤变II+级的三年累积发病率为17.0%(95%置信区间12.1%至22.0%)。那些检测呈阴性/阳性(3.4%,0.1%至6.8%)、阳性/阴性(1.2%,-0.2%至2.5%)和阴性/阴性(0.5%,0.1%至0.9%)的女性风险显著较低。对于任何致癌HPV基因型检测呈阳性两次(相同基因型或不同基因型)与相同致癌基因型检测呈阳性两次之间,宫颈上皮内瘤变II+级的累积发病率差异不大(分别为17.0%和21.3%)。HPV 16的短期持续存在强烈预示宫颈上皮内瘤变II+级,三年累积发病率为40.8%(26.4%至55.1%)。对于II+级的五年累积发病率以及III+级的三年和五年累积发病率,观察到类似模式。
普遍检测到的致癌性HPV感染的短期持续存在,尤其是HPV 16,强烈预示在接下来几年中随后被诊断为宫颈上皮内瘤变II+级。