Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.
PLoS One. 2009 Aug 14;4(8):e6642. doi: 10.1371/journal.pone.0006642.
Early diagnosis of sepsis enables timely resuscitation and antibiotics and prevents subsequent morbidity and mortality. Clinical approaches relying on point-in-time analysis of vital signs or lab values are often insensitive, non-specific and late diagnostic markers of sepsis. Exploring otherwise hidden information within intervals-in-time, heart rate variability (HRV) has been documented to be both altered in the presence of sepsis, and correlated with its severity. We hypothesized that by continuously tracking individual patient HRV over time in patients as they develop sepsis, we would demonstrate reduced HRV in association with the onset of sepsis.
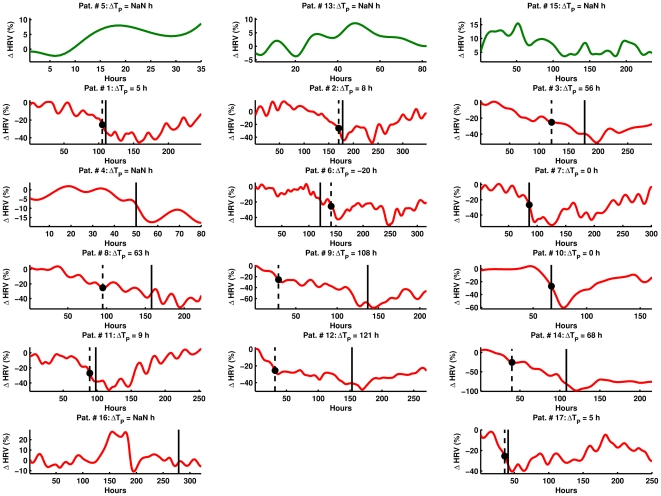
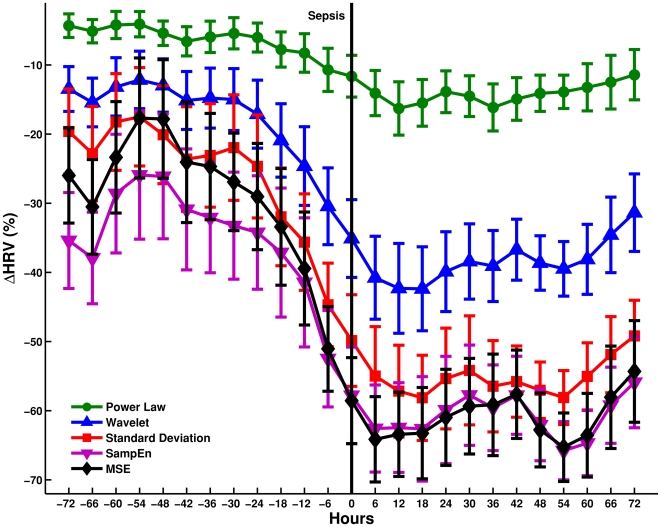
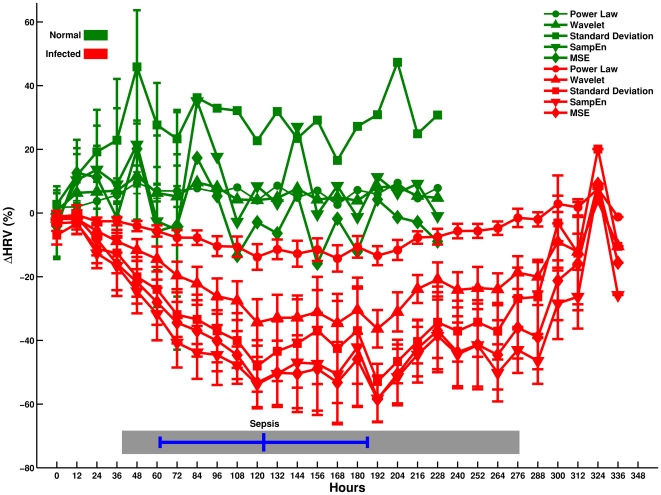
METHODOLOGY/PRINCIPAL FINDINGS: We monitored heart rate continuously in adult bone marrow transplant (BMT) patients (n = 21) beginning a day before their BMT and continuing until recovery or withdrawal (12+/-4 days). We characterized HRV continuously over time with a panel of time, frequency, complexity, and scale-invariant domain techniques. We defined baseline HRV as mean variability for the first 24 h of monitoring and studied individual and population average percentage change (from baseline) over time in diverse HRV metrics, in comparison with the time of clinical diagnosis and treatment of sepsis (defined as systemic inflammatory response syndrome along with clinically suspected infection requiring treatment). Of the 21 patients enrolled, 4 patients withdrew, leaving 17 patients who completed the study. Fourteen patients developed sepsis requiring antibiotic therapy, whereas 3 did not. On average, for 12 out of 14 infected patients, a significant (25%) reduction prior to the clinical diagnosis and treatment of sepsis was observed in standard deviation, root mean square successive difference, sample and multiscale entropy, fast Fourier transform, detrended fluctuation analysis, and wavelet variability metrics. For infected patients (n = 14), wavelet HRV demonstrated a 25% drop from baseline 35 h prior to sepsis on average. For 3 out of 3 non-infected patients, all measures, except root mean square successive difference and entropy, showed no significant reduction. Significant correlation was present amongst these HRV metrics for the entire population.
CONCLUSIONS/SIGNIFICANCE: Continuous HRV monitoring is feasible in ambulatory patients, demonstrates significant HRV alteration in individual patients in association with, and prior to clinical diagnosis and treatment of sepsis, and merits further investigation as a means of providing early warning of sepsis.
早期诊断脓毒症可实现及时复苏和应用抗生素,从而预防后续发病率和死亡率。基于生命体征或实验室检查的时间点分析的临床方法往往不敏感、特异性差,是脓毒症的晚期诊断标志物。心率变异性(HRV)在时间间隔内探索隐藏的信息,已被证明在脓毒症存在时发生改变,并与严重程度相关。我们假设,通过在患者发生脓毒症时连续跟踪个体患者的 HRV 随时间的变化,我们将证明 HRV 降低与脓毒症的发生有关。
方法/主要发现:我们连续监测了 21 名成人骨髓移植(BMT)患者(n=21)的心率,从他们进行 BMT 的前一天开始,一直持续到恢复或退出(12+/-4 天)。我们使用一系列时间、频率、复杂性和标度不变域技术连续监测 HRV。我们将前 24 小时的平均变异性定义为基线 HRV,并研究了不同 HRV 指标的个体和群体平均百分比变化(相对于基线),与临床诊断和治疗脓毒症的时间(定义为全身炎症反应综合征以及伴有临床疑似感染需要治疗的情况)进行比较。在纳入的 21 名患者中,4 名患者退出,17 名患者完成了研究。14 名患者发生脓毒症需要抗生素治疗,而 3 名患者没有。平均而言,对于 14 名感染患者中的 12 名,在临床诊断和治疗脓毒症之前观察到标准偏差、均方根连续差异、样本和多尺度熵、快速傅里叶变换、去趋势波动分析和小波变异性指标显著降低(25%)。对于感染患者(n=14),平均在脓毒症前 35 小时,小波 HRV 从基线下降了 25%。对于 3 名非感染患者,除均方根连续差异和熵外,所有指标均未显示出显著降低。对于整个人群,这些 HRV 指标之间存在显著相关性。
结论/意义:连续 HRV 监测在门诊患者中是可行的,在个体患者中显示出与临床诊断和治疗脓毒症相关的显著 HRV 改变,并且在脓毒症的早期预警方面值得进一步研究。