Levy Wayne C, Lee Kerry L, Hellkamp Anne S, Poole Jeanne E, Mozaffarian Dariush, Linker David T, Maggioni Aldo P, Anand Inder, Poole-Wilson Philip A, Fishbein Daniel P, Johnson George, Anderson Jill, Mark Daniel B, Bardy Gust H
Division of Cardiology, University of Washington, Box 356422, 1959 NE Pacific St, Seattle, WA 98195, USA.
Circulation. 2009 Sep 8;120(10):835-42. doi: 10.1161/CIRCULATIONAHA.108.816884. Epub 2009 Aug 24.
Although implantable cardioverter-defibrillator (ICD) therapy reduces mortality in moderately symptomatic heart failure patients with an ejection fraction <or=35%, many such patients do not require ICD shocks over long-term follow-up.
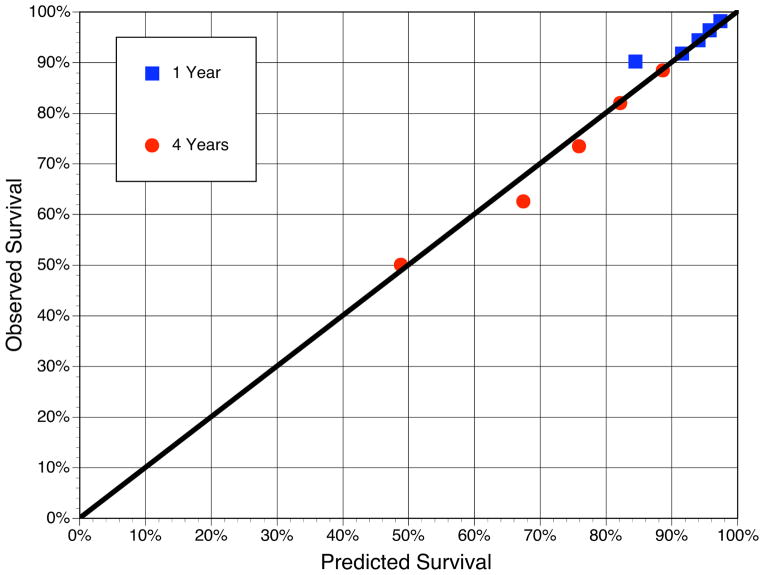
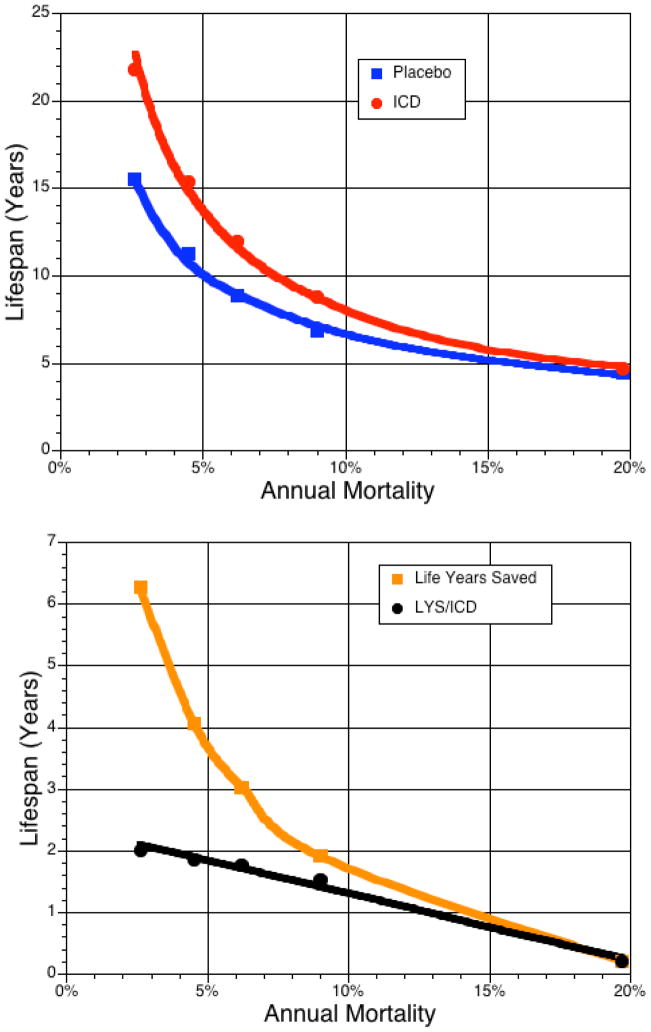
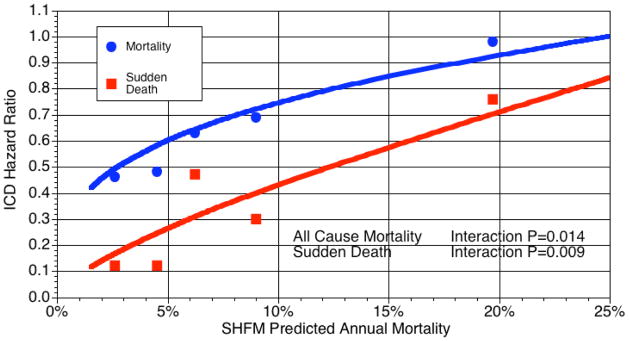
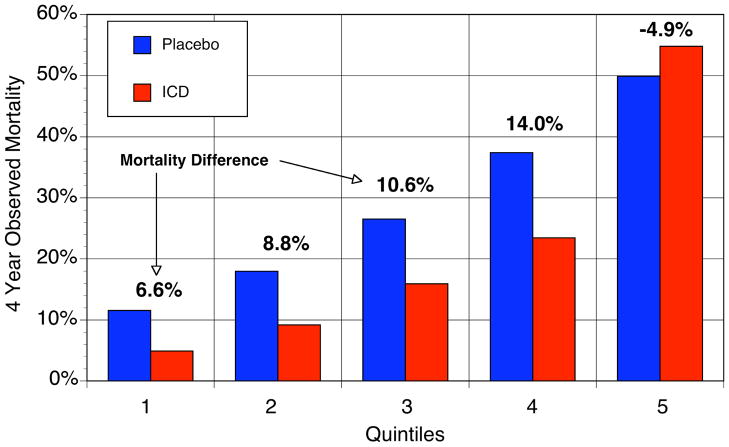
Using a modification of a previously validated risk prediction model based on routine clinical variables, we examined the relationship between baseline predicted mortality risk and the relative and absolute survival benefits of ICD treatment in the primary prevention Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). In the placebo arm, predicted 4-year mortality grouped into 5 equal-sized risk groups varied from 12% to 50% (c statistic=0.71), whereas the proportion of SCD in those same risk groups decreased from 52% to 24% of all deaths. ICD treatment decreased relative risk of SCD by 88% in the lowest-risk group versus 24% in the highest-risk group (P=0.009 for interaction) and decreased relative risk of total mortality by 54% in the lowest-risk group versus no benefit (2%) in the highest-risk group (P=0.014 for interaction). Absolute 4-year mortality reductions were 6.6%, 8.8%, 10.6%, 14.0%, and -4.9% across risk quintiles. In highest-risk patients (predicted annual mortality >20%), no benefit of ICD treatment was seen. Projected over each patient's predicted lifespan, ICD treatment added 6.3, 4.1, 3.0, 1.9, and 0.2 additional years of life in the lowest- to highest-risk groups, respectively.
A clinical risk prediction model identified subsets of moderately symptomatic heart failure patients in SCD-HeFT in whom single-lead ICD therapy was of no benefit and other subsets in which benefit was substantial.
尽管植入式心脏复律除颤器(ICD)治疗可降低射血分数≤35%的中度症状性心力衰竭患者的死亡率,但许多此类患者在长期随访中并不需要ICD电击治疗。
我们基于常规临床变量对先前验证的风险预测模型进行修改,在心力衰竭试验(SCD-HeFT)的一级预防心脏性猝死研究中,研究了基线预测死亡风险与ICD治疗的相对和绝对生存获益之间的关系。在安慰剂组中,预测4年死亡率分为5个等风险组,从12%到50%不等(c统计量=0.71),而这些相同风险组中的心源性猝死比例从所有死亡的52%降至24%。ICD治疗使最低风险组的心源性猝死相对风险降低88%,而最高风险组降低24%(交互作用P=0.009),使最低风险组的总死亡相对风险降低54%,而最高风险组无获益(2%)(交互作用P=0.014)。4年绝对死亡率降低分别为6.6%、8.8%、10.6%、14.0%和-4.9%。在最高风险患者(预测年死亡率>20%)中,未观察到ICD治疗的获益。根据每位患者的预测寿命推算,ICD治疗在最低至最高风险组中分别增加了6.3、4.1、3.0、1.9和0.2年的生命。
临床风险预测模型在SCD-HeFT中识别出了单腔ICD治疗无获益的中度症状性心力衰竭患者亚组以及获益显著的其他亚组。