Papavassiliu Theano, Germans Tjeerd, Flüchter Stephan, Doesch Christina, Suriyakamar Anton, Haghi Dariusch, Süselbeck Tim, Wolpert Christian, Dinter Dietmar, Schoenberg Stefan O, van Rossum Albert C, Borggrefe Martin
1st Department of Medicine-Cardiology, University Hospital of Mannheim, Mannheim, Germany.
J Cardiovasc Magn Reson. 2009 Sep 9;11(1):34. doi: 10.1186/1532-429X-11-34.
We sought to evaluate the relation between atrial fibrillation (AF) and the extent of myocardial scarring together with left ventricular (LV) and atrial parameters assessed by late gadolinium-enhancement (LGE) cardiovascular magnetic resonance (CMR) in patients with hypertrophic cardiomyopathy (HCM).
AF is the most common arrhythmia in HCM. Myocardial scarring is also identified frequently in HCM. However, the impact of myocardial scarring assessed by LGE CMR on the presence of AF has not been evaluated yet.
87 HCM patients underwent LGE CMR, echocardiography and regular ECG recordings. LV function, volumes, myocardial thickness, left atrial (LA) volume and the extent of LGE, were assessed using CMR and correlated to AF. Additionally, the presence of diastolic dysfunction and mitral regurgitation were obtained by echocardiography and also correlated to AF.
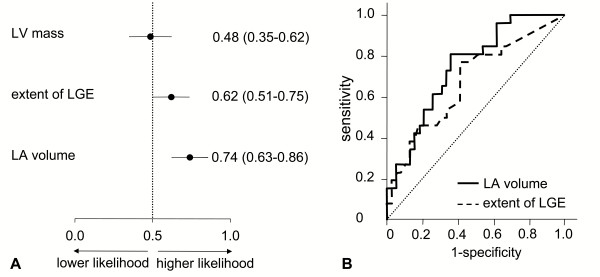
Episodes of AF were documented in 37 patients (42%). Indexed LV volumes and mass were comparable between HCM patients with and without AF. However, indexed LA volume was significantly higher in HCM patients with AF than in HCM patients without AF (68 +/- 24 ml.m-2 versus 46 +/- 18 ml.m-2, p = 0.0002, respectively). The mean extent of LGE was higher in HCM patients with AF than those without AF (12.4 +/- 14.5% versus 6.0 +/- 8.6%, p = 0.02). When adjusting for age, gender and LV mass, LGE and indexed LA volume significantly correlated to AF (r = 0.34, p = 0.02 and r = 0.42, p < 0.001 respectively). By echocardiographic examination, LV diastolic dysfunction was evident in 35 (40%) patients. Mitral regurgitation greater than II was observed in 12 patients (14%). Multivariate analysis demonstrated that LA volume and presence of diastolic dysfunction were the only independent determinant of AF in HCM patients (p = 0.006, p = 0.01 respectively). Receiver operating characteristic curve analysis indicated good predictive performance of LA volume and LGE (AUC = 0.74 and 0.64 respectively) with respect to AF.
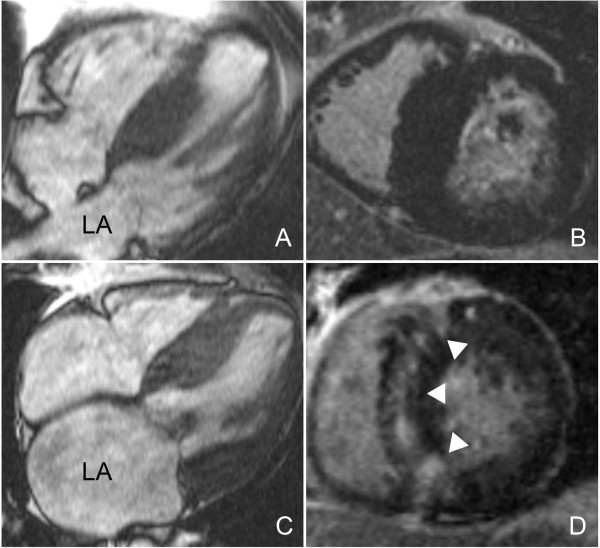
HCM patients with AF display significantly more LGE than HCM patients without AF. However, the extent of LGE is inferior to the LA size for predicting AF prevalence. LA dilation is the strongest determinant of AF in HCM patients, and is related to the extent of LGE in the LV, irrespective of LV mass.
我们旨在评估肥厚型心肌病(HCM)患者中房颤(AF)与心肌瘢痕范围以及通过延迟钆增强(LGE)心血管磁共振(CMR)评估的左心室(LV)和心房参数之间的关系。
房颤是HCM中最常见的心律失常。心肌瘢痕在HCM中也经常被发现。然而,LGE CMR评估的心肌瘢痕对房颤存在的影响尚未得到评估。
87例HCM患者接受了LGE CMR、超声心动图检查和常规心电图记录。使用CMR评估LV功能、容积、心肌厚度、左心房(LA)容积和LGE范围,并与房颤相关联。此外,通过超声心动图检查获得舒张功能障碍和二尖瓣反流的情况,并也与房颤相关联。
37例患者(42%)记录到房颤发作。有房颤和无房颤的HCM患者的左心室指数容积和质量相当。然而,有房颤的HCM患者的左心房指数容积显著高于无房颤的HCM患者(分别为68±24 ml.m-2和46±18 ml.m-2,p = 0.0002)。有房颤的HCM患者的LGE平均范围高于无房颤的患者(12.4±14.5%对6.0±8.6%,p = 0.02)。在调整年龄、性别和左心室质量后,LGE和左心房指数容积与房颤显著相关(r = 0.34,p = 0.02和r = 0.42,p < 0.001)。通过超声心动图检查,35例(40%)患者存在明显的左心室舒张功能障碍。12例患者(14%)观察到二尖瓣反流大于II级。多因素分析表明,左心房容积和舒张功能障碍的存在是HCM患者房颤的唯一独立决定因素(分别为p = 0.006,p = 0.01)。受试者工作特征曲线分析表明,左心房容积和LGE对房颤具有良好的预测性能(AUC分别为0.74和0.64)。
有房颤的HCM患者比无房颤的HCM患者表现出明显更多的LGE。然而,LGE范围在预测房颤患病率方面不如左心房大小。左心房扩张是HCM患者房颤的最强决定因素,并且与左心室LGE范围相关,与左心室质量无关。