Douglas Ian J, Evans Stephen J, Pocock Stuart, Smeeth Liam
Non Communicable Disease Unit, Department of Epidemiology & Population Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
PLoS Med. 2009 Sep;6(9):e1000154. doi: 10.1371/journal.pmed.1000154. Epub 2009 Sep 29.
The results of clinical trials have suggested that the thiazolidinedione antidiabetic agents rosiglitazone and pioglitazone are associated with an increased risk of fractures, but such studies had limited power. The increased risk in these trials appeared to be limited to women and mainly involved fractures of the arm, wrist, hand, or foot: risk patterns that could not be readily explained. Our objective was to further investigate the risk of fracture associated with thiazolidinedione use.
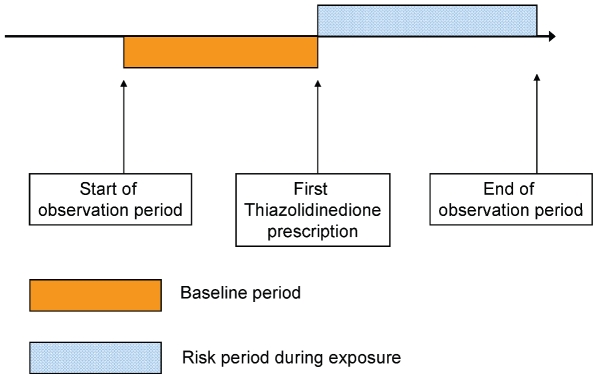
The self-controlled case-series design was used to compare rates of fracture during thiazolidinedione exposed and unexposed periods and thus estimate within-person rate ratios. We used anonymised primary care data from the United Kingdom General Practice Research Database (GPRD). All patients aged 40 y or older with a recorded fracture and at least one prescription for a thiazolidinedione were included (n = 1,819). We found a within-person rate ratio of 1.43 (95% confidence interval [CI] 1.25-1.62) for fracture at any site comparing exposed with unexposed periods among patients prescribed any thiazolidinedione. This association was similar in men and women and in patients treated with either rosiglitazone or pioglitazone. The increased risk was also evident at a range of fracture sites, including hip, spine, arm, foot, wrist, or hand. The risk increased with increasing duration of thiazolidinedione exposure: rate ratio 2.00 (95% CI 1.48-2.70) for 4 y or more of exposure.
Within individuals who experience a fracture, fracture risk is increased during periods of exposure to thiazolidinediones (both rosiglitazone and pioglitazone) compared with unexposed periods. The increased risk is observed in both men and women and at a range of fracture sites. The risk also increases with longer duration of use.
临床试验结果表明,噻唑烷二酮类抗糖尿病药物罗格列酮和吡格列酮与骨折风险增加有关,但此类研究的效力有限。这些试验中增加的风险似乎仅限于女性,且主要涉及手臂、手腕、手部或足部骨折:这些风险模式难以轻易解释。我们的目的是进一步研究使用噻唑烷二酮类药物相关的骨折风险。
采用自身对照病例系列设计,比较使用噻唑烷二酮类药物期间和未使用期间的骨折发生率,从而估算个体内发生率比。我们使用了来自英国全科医疗研究数据库(GPRD)的匿名初级保健数据。纳入了所有年龄在40岁及以上、有骨折记录且至少有一张噻唑烷二酮类药物处方的患者(n = 1819)。我们发现,在开具任何噻唑烷二酮类药物的患者中,比较使用药物期间和未使用期间,任何部位骨折的个体内发生率比为1.43(95%置信区间[CI] 1.25 - 1.62)。男性和女性以及使用罗格列酮或吡格列酮治疗的患者中,这种关联相似。在一系列骨折部位,包括髋部、脊柱、手臂、足部、手腕或手部,增加的风险也很明显。骨折风险随着噻唑烷二酮类药物暴露时间的延长而增加:暴露4年或更长时间的发生率比为2.00(95% CI 1.48 - 2.70)。
在经历过骨折的个体中,与未使用噻唑烷二酮类药物期间相比,使用噻唑烷二酮类药物(罗格列酮和吡格列酮)期间骨折风险增加。男性和女性以及在一系列骨折部位均观察到增加的风险。风险也随着用药时间延长而增加。