Department of Internal Medicine, Section on Hematology and Oncology, Wake Forest University School of Medicine, Winston-Salem, NC, USA.
J Hematol Oncol. 2009 Oct 24;2:44. doi: 10.1186/1756-8722-2-44.
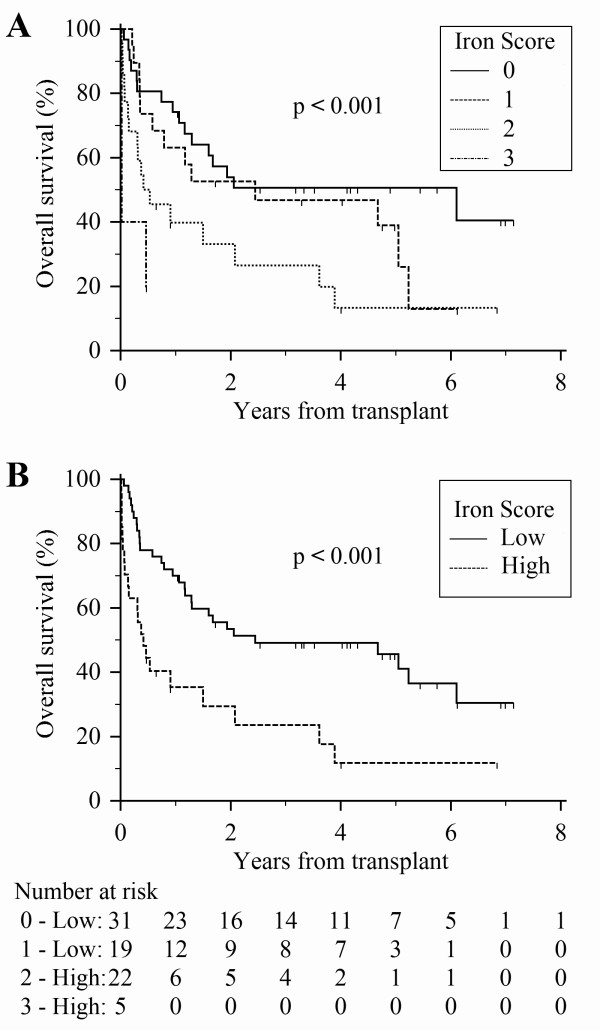
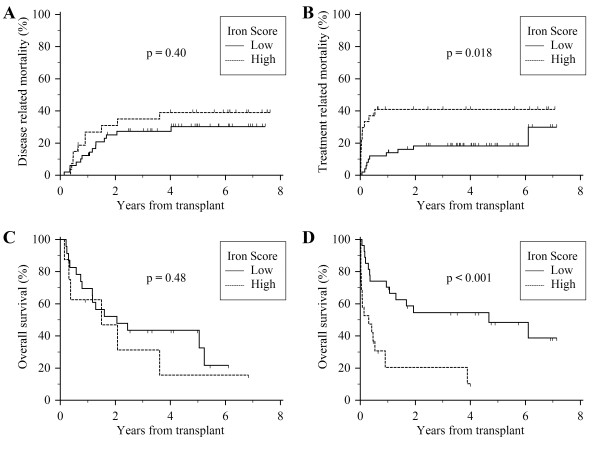
Recent studies have suggested that the presence of iron overload prior to stem cell transplantation is associated with decreased survival. Within these studies, the criteria used to define iron overload have varied considerably. Given the lack of consensus regarding the definition of iron overload in the transplant setting, we sought to methodically examine iron status among transplant patients. We studied 78 consecutive patients at risk for transfusion-related iron overload (diagnoses included AML, ALL, MDS, and aplastic anemia) who received either autologous or allogeneic stem cell transplant. Multiple measures of iron status were collected prior to transplantation and examined for their association with survival. Using this data, three potentially prognostic iron measures were identified and incorporated into a rational and unified scoring system. The resulting Transplant Iron Score assigns a point for each of the following variables: (1) greater than 25 red cell units transfused prior to transplantation; (2) serum ferritin > 1000 ng/ml; and (3) a semi-quantitative bone marrow iron stain of 6+. In our cohort, the score (range 0 to 3) was more closely associated with survival than any available single iron parameter. In multivariate analysis, we observed an independent effect of iron overload on transplant survival (p = 0.01) primarily attributable to an increase in early treatment-related deaths (p = 0.02) and lethal infections. In subgroup analysis, the predictive power of the iron score was most pronounced among allogeneic transplant patients, where a high score (> or = 2) was associated with a 50% absolute decrease in survival at one year. In summary, our results lend further credence to the notion that iron overload prior to transplant is detrimental and suggest iron overload may predispose to a higher rate of lethal infections.
最近的研究表明,干细胞移植前铁过载与生存率降低有关。在这些研究中,用于定义铁过载的标准差异很大。鉴于在移植环境中缺乏关于铁过载定义的共识,我们试图系统地检查移植患者的铁状况。我们研究了 78 例有输血相关铁过载风险的连续患者(诊断包括 AML、ALL、MDS 和再生障碍性贫血),他们接受了自体或同种异体干细胞移植。在移植前收集了多种铁状态指标,并检查了它们与生存率的关系。利用这些数据,确定了三种潜在的预后铁指标,并将其纳入一个合理和统一的评分系统。由此产生的移植铁评分对以下每个变量赋予一个分数:(1)移植前输注的红细胞单位数大于 25;(2)血清铁蛋白> 1000ng/ml;(3)半定量骨髓铁染色为 6+。在我们的队列中,评分(范围 0 至 3)与生存率的相关性比任何可用的单一铁参数都更密切。在多变量分析中,我们观察到铁过载对移植生存率的独立影响(p = 0.01),主要归因于治疗相关早期死亡(p = 0.02)和致命感染的增加。在亚组分析中,铁评分的预测能力在同种异体移植患者中最为明显,其中高评分(> = 2)与一年时生存率绝对下降 50%相关。总之,我们的结果进一步证实了移植前铁过载有害的观点,并表明铁过载可能导致致命感染的发生率增加。