Srivastava Rajendu, Berry Jay G, Hall Matt, Downey Earl C, O'Gorman Molly, Dean J Michael, Barnhart Douglas C
Division of Inpatient Medicine, Department of Pediatrics, University of Utah Health Sciences Center, Salt Lake City, UT, USA.
BMJ. 2009 Nov 18;339:b4411. doi: 10.1136/bmj.b4411.
To examine the impact of fundoplication on reflux related hospital admissions for children with neurological impairment.
Retrospective, observational cohort study. Setting 42 children's hospitals in the United States.
3721 children with neurological impairment born between 2000 and 2005 who had at least one hospital admission at a study hospital before their fundoplication.
Fundoplication.
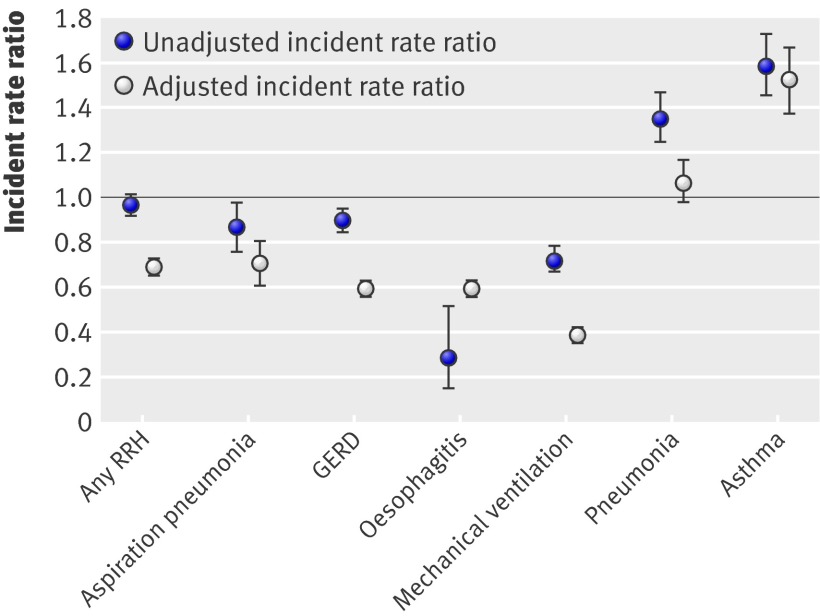
Incident rate ratio for reflux related hospital admissions, defined as the post-fundoplication admission rate divided by the pre-fundoplication admission rate.
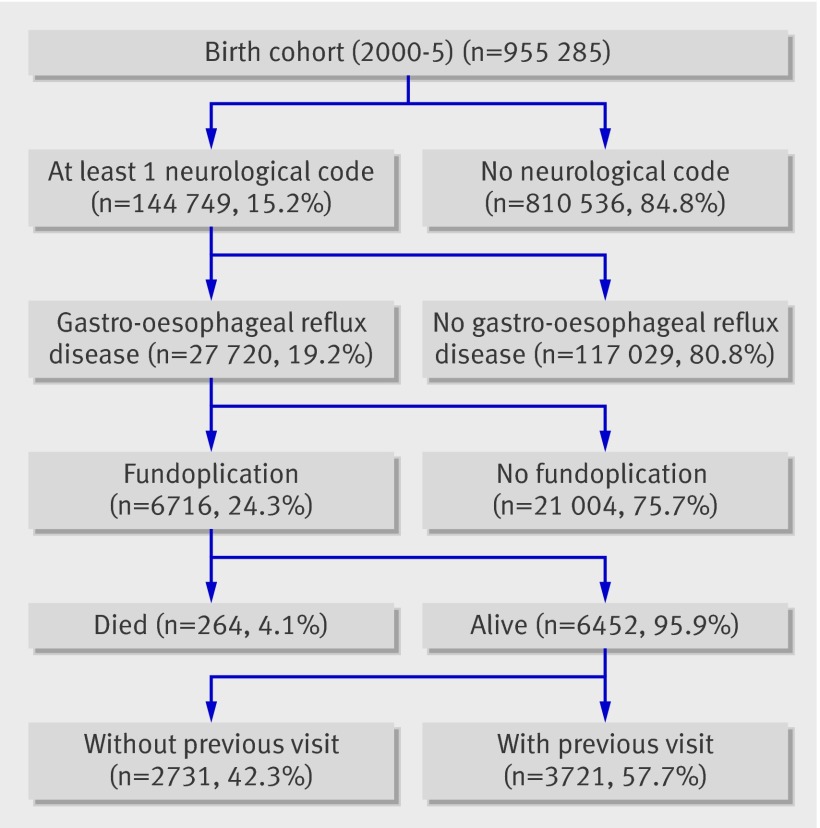
Of the 955 285 children born during the study period, 144,749 (15%) had neurological impairment. Of these, 27,720 (19%) were diagnosed as having gastro-oesophageal reflux disease, of whom 6716 (24%) had a fundoplication. Of these, 3721 (55%) had at least one previous hospital admission and were included in the study cohort. After fundoplication, hospital admissions decreased for any reflux related cause (incident rate ratio 0.69, 95% confidence interval 0.67 to 0.72; P<0.01), aspiration pneumonia (0.71, 0.62 to 0.81; P<0.01), gastro-oesophageal reflux disease (0.60, 0.57 to 0.63; P<0.01), and mechanical ventilation (0.40, 0.37 to 0.43; P<0.01), after adjustment for other patient and hospital related factors that may influence reflux related hospital admissions. Hospital admissions increased for asthma (incident rate ratio 1.52, 1.38 to 1.67; P<0.01) and remained constant for pneumonia (1.07, 0.98 to 1.17; P=0.16). Conclusions Children with neurological impairment who have fundoplication had reduced short term reflux related hospital admissions for aspiration pneumonia, gastro-oesophageal reflux disease, and mechanical ventilation. However, admissions for pneumonia remained constant and those for asthma increased after fundoplication. Comparative effectiveness data for other treatments (such as gastrojejunal feeding tubes) are unknown.
探讨胃底折叠术对神经功能障碍儿童反流相关住院情况的影响。
回顾性观察队列研究。研究地点为美国42家儿童医院。
3721名2000年至2005年出生的神经功能障碍儿童,在接受胃底折叠术之前至少在一家研究医院住院过一次。
胃底折叠术。
反流相关住院的发病率比,定义为胃底折叠术后住院率除以胃底折叠术前住院率。
在研究期间出生的955285名儿童中,144749名(15%)有神经功能障碍。其中,27720名(19%)被诊断为患有胃食管反流病,其中6716名(24%)接受了胃底折叠术。其中,3721名(55%)此前至少有一次住院,并被纳入研究队列。胃底折叠术后,因任何反流相关原因导致的住院人数减少(发病率比0.69,95%置信区间0.67至0.72;P<0.01),吸入性肺炎(0.71,0.62至0.81;P<0.01)、胃食管反流病(0.60,0.57至0.63;P<0.01)和机械通气(0.40,0.37至0.43;P<0.01),在对可能影响反流相关住院的其他患者和医院相关因素进行调整后。哮喘导致的住院人数增加(发病率比1.52,1.38至1.67;P<0.01),肺炎导致的住院人数保持不变(1.07,0.98至1.17;P=0.16)。结论接受胃底折叠术的神经功能障碍儿童因吸入性肺炎、胃食管反流病和机械通气导致的短期反流相关住院人数减少。然而,胃底折叠术后肺炎导致的住院人数保持不变,哮喘导致的住院人数增加。其他治疗方法(如胃空肠喂养管)的比较有效性数据尚不清楚。