Hippisley-Cox Julia, Coupland Carol
Division of Primary Care, Tower Building, University Park, Nottingham NG2 7RD.
BMJ. 2009 Nov 19;339:b4229. doi: 10.1136/bmj.b4229.
To develop and validate two new fracture risk algorithms (QFractureScores) for estimating the individual risk of osteoporotic fracture or hip fracture over 10 years.
Prospective open cohort study with routinely collected data from 357 general practices to develop the scores and from 178 practices to validate the scores.
General practices in England and Wales.
1 183 663 women and 1 174 232 men aged 30-85 in the derivation cohort, who contributed 7 898 208 and 8 049 306 person years of observation, respectively. There were 24 350 incident diagnoses of osteoporotic fracture in women and 7934 in men, and 9302 incident diagnoses of hip fracture in women and 5424 in men.
First (incident) diagnosis of osteoporotic fracture (vertebral, distal radius, or hip) and incident hip fracture recorded in general practice records.
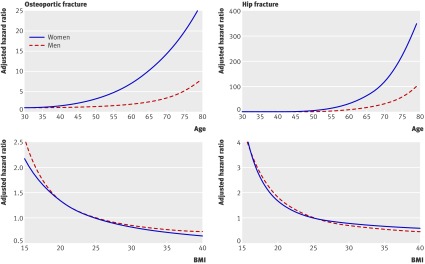
Use of hormone replacement therapy (HRT), age, body mass index (BMI), smoking status, recorded alcohol use, parental history of osteoporosis, rheumatoid arthritis, cardiovascular disease, type 2 diabetes, asthma, tricyclic antidepressants, corticosteroids, history of falls, menopausal symptoms, chronic liver disease, gastrointestinal malabsorption, and other endocrine disorders were significantly and independently associated with risk of osteoporotic fracture in women. Some variables were significantly associated with risk of osteoporotic fracture but not with risk of hip fracture. The predictors for men for osteoporotic and hip fracture were age, BMI, smoking status, recorded alcohol use, rheumatoid arthritis, cardiovascular disease, type 2 diabetes, asthma, tricyclic antidepressants, corticosteroids, history of falls, and liver disease. The hip fracture algorithm had the best performance among men and women. It explained 63.94% of the variation in women and 63.19% of the variation in men. The D statistic values for discrimination were highest for hip fracture in women (2.73) and men (2.68) and were over twice the magnitude of the corresponding values for osteoporotic fracture. The ROC statistics for hip fracture were also high: 0.89 in women and 0.86 for men versus 0.79 and 0.69, respectively, for the osteoporotic fracture outcome. The algorithms were well calibrated with predicted risks closely matching observed risks. The QFractureScore for hip fracture also had good performance for discrimination and calibration compared with the FRAX (fracture risk assessment) algorithm.
These new algorithms can predict risk of fracture in primary care populations in the UK without laboratory measurements and are therefore suitable for use in both clinical settings and for self assessment (www.qfracture.org). QFractureScores could be used to identify patients at high risk of fracture who might benefit from interventions to reduce their risk.
开发并验证两种新的骨折风险算法(QFractureScores),以评估个体未来10年内发生骨质疏松性骨折或髋部骨折的风险。
前瞻性开放队列研究,利用从357家全科诊所常规收集的数据来开发评分系统,并从178家诊所收集数据进行验证。
英格兰和威尔士的全科诊所。
推导队列中有1183663名年龄在30 - 85岁之间的女性和1174232名男性,分别贡献了7898208和8049306人年的观察数据。女性中有24350例骨质疏松性骨折的新发诊断病例,男性中有7934例;女性中有9302例髋部骨折的新发诊断病例,男性中有5424例。
全科医疗记录中记录的骨质疏松性骨折(椎体、桡骨远端或髋部)的首次(新发)诊断以及髋部骨折的新发诊断。
在女性中,使用激素替代疗法(HRT)、年龄、体重指数(BMI)、吸烟状况、记录的饮酒情况、骨质疏松症家族史、类风湿关节炎、心血管疾病、2型糖尿病、哮喘、三环类抗抑郁药、皮质类固醇、跌倒史、绝经症状、慢性肝病、胃肠道吸收不良以及其他内分泌疾病与骨质疏松性骨折风险显著且独立相关。一些变量与骨质疏松性骨折风险显著相关,但与髋部骨折风险无关。男性骨质疏松性骨折和髋部骨折的预测因素包括年龄、BMI、吸烟状况、记录的饮酒情况、类风湿关节炎、心血管疾病、2型糖尿病、哮喘、三环类抗抑郁药、皮质类固醇、跌倒史和肝病。髋部骨折算法在男性和女性中表现最佳。它解释了女性中63.94%的变异和男性中63.19%的变异。女性髋部骨折的鉴别D统计值最高(2.73),男性为(2.68),是骨质疏松性骨折相应值的两倍多。髋部骨折的ROC统计值也很高:女性为0.89,男性为0.86,而骨质疏松性骨折结果的相应值分别为0.79和0.69。这些算法校准良好,预测风险与观察到的风险紧密匹配。与FRAX(骨折风险评估)算法相比,髋部骨折的QFractureScore在鉴别和校准方面也表现良好。
这些新算法无需实验室检测即可预测英国基层医疗人群的骨折风险,因此适用于临床环境和自我评估(www.qfracture.org)。QFractureScores可用于识别骨折高风险患者,这些患者可能从降低风险的干预措施中获益。