Bungard Tammy J, Gardner Leslie, Archer Stephen L, Hamilton Peter, Ritchie Bruce, Tymchak Wayne, Tsuyuki Ross T
Open Med. 2009 Feb 2;3(1):e16-21.
Anticoagulation management services (AMSs) are widely used for anticoagulation management in many countries. Our AMS is a pharmacist-run ambulatory clinic with a physician advisory committee that manages patients referred with complicated anticoagulation histories. This paper assesses the adequacy of anticoagulation, rates of anticoagulant-related events and associated health care resource utilization for patients before and after referral to our AMS.
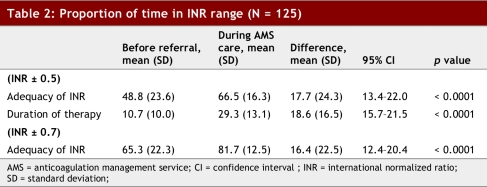
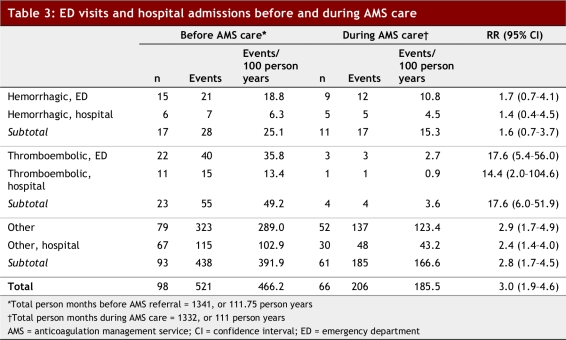
Consecutive patients referred to the AMS with 4 months of prior anticoagulation management who also had anticoagulation management for 4 months within the AMS were included in the evaluation. The primary endpoint was adequacy of anticoagulation (target international normalized ratio [INR] +/- 0.5). Secondary outcomes included adverse events requiring an emergency department (ED) visit or hospital stay. These were classified by International Classification of Diseases (ICD) codes as thromboembolic, hemorrhagic, or non-anticoagulant related. Health care system resource consumption data were collected as number of hours spent in an ED and hospitalization costs.
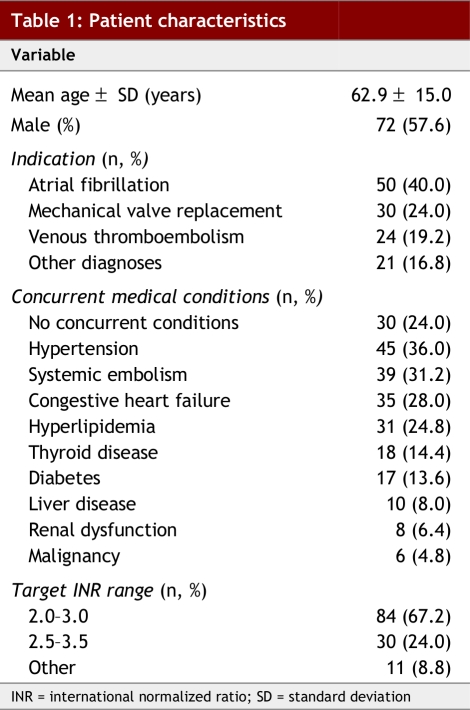
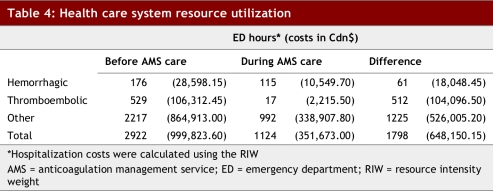
A total of 125 patients were included: 57.6% were male, with a mean age of 62.9 (standard deviation [SD]) +/- 15.0 years. Indications for warfarin therapy were atrial fibrillation (40.0%), mechanical valve replacement (24.0%) and venous thromboembolism (19.2%). The adequacy of anticoagulant control was significantly greater during AMS care compared with the period before referral; patients were in the target INR range 66.5% versus 48.8% of the time, respectively (95% confidence interval [CI] 13.4%-22.0%; p < 0.0001). The relative risk of a thromboembolic event before referral to AMS care was 17.6 (95% CI 6.0-51.9; p < 0.0001), while the relative risk of a hemorrhagic event before AMS care was 1.6 (95% CI 0.7-3.7; p = 0.25). During AMS care, savings included 572 hours in the ED and Cdn$122,145.40 in hospitalization costs.
A pharmacist-directed, physician-supported AMS program achieved significantly better INR control and reduced rates of thromboembolic complications compared with standard care. Resource utilization was substantially reduced during AMS care.
抗凝管理服务(AMSs)在许多国家被广泛用于抗凝管理。我们的AMS是一个由药剂师管理的门诊诊所,设有一个医师咨询委员会,负责管理有复杂抗凝治疗史的转诊患者。本文评估了转诊至我们的AMS前后患者的抗凝充分性、抗凝相关事件发生率以及相关医疗资源的利用情况。
连续纳入转诊至AMS且此前有4个月抗凝管理经历、在AMS内也接受了4个月抗凝管理的患者进行评估。主要终点是抗凝充分性(目标国际标准化比值[INR]±0.5)。次要结局包括需要急诊就诊或住院的不良事件。这些事件根据国际疾病分类(ICD)编码分为血栓栓塞性、出血性或非抗凝相关。收集医疗系统资源消耗数据,包括在急诊花费的小时数和住院费用。
共纳入125例患者:57.6%为男性,平均年龄62.9(标准差[SD])±15.0岁。华法林治疗的适应证为房颤(40.0%)、机械瓣膜置换(24.0%)和静脉血栓栓塞(19.2%)。与转诊前相比,在AMS护理期间抗凝控制的充分性显著更高;患者分别有66.5%和48.8%的时间处于目标INR范围内(95%置信区间[CI] 13.4%-22.0%;p<0.0001)。转诊至AMS护理前血栓栓塞事件的相对风险为17.6(95%CI 6.0-51.9;p<0.0001),而在AMS护理前出血事件的相对风险为1.6(95%CI 0.7-3.7;p = 0.25)。在AMS护理期间,节省了572小时的急诊时间和122,145.40加元的住院费用。
与标准护理相比,由药剂师主导、医师支持的AMS项目实现了显著更好的INR控制,并降低了血栓栓塞并发症的发生率。在AMS护理期间,资源利用大幅减少。