Hospital Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain.
Eur J Med Res. 2009 Nov 24;14 Suppl 3(Suppl 3):30-5. doi: 10.1186/2047-783x-14-s3-30.
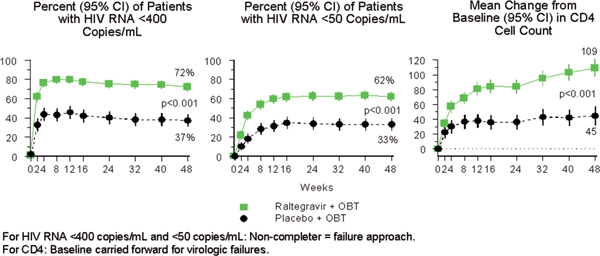
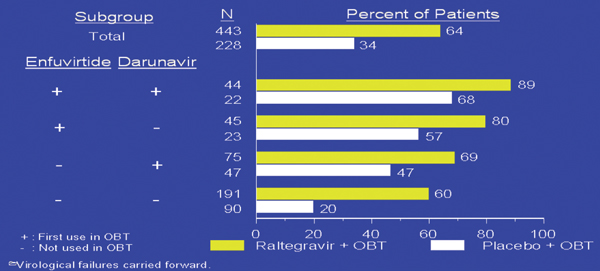
Raltegravir, the first approved HIV-1 integrase inhibitor, is able to block the strand transfer step of the HIV proviral DNA integration process into the cellular host DNA. The selected dosage for the pivotal phase III studies (subsequently approved by the regulatory agencies) was 400mg bid by oral route with or without food. Raltegravir has a week effect (either inhibition or induction) on the hepatic cytochrone P450 activity. There is not need of dose adjustments in renal insufficiency or in mild-to-moderate hepatic impairment. The emerging paradigm in the field of salvage therapy was to achieve a viral load below limit of detection in almost all patients. Pretty soon it became apparent that this was feasible in more than 70-90% of patients. Raltegravir proved to be pivotal for this new paradigm. Raltegravir vs placebo both with an optimized background therapy has been tested for salvage therapy in the 005 and in the BENCHMRK studies (018 and 019). In all three studies proved to be superior to the placebo at 24, 48 and 96 weeks. Tolerance was remarkably good and virological failure was often associated with selection of integrase gene resistance mutations following the Y143C/H/R, Q148H/K/R o less frequently the NI55H paths. Finally, in the two SWITCHMRK studies non-inferiority vs Lopinavir/r could not be demonstrated in virogically suppressed patients with an stable cART containing Lopinavir/r. Most likely explanation was the presence of archived resistance mutationts to background therapy leading to a functional monotherapy with raltegravir.
拉替拉韦,第一个被批准的 HIV-1 整合酶抑制剂,能够阻断 HIV 前病毒 DNA 整合到细胞宿主 DNA 的链转移步骤。关键性的 III 期研究(随后被监管机构批准)选定的剂量为 400mg bid,口服,有或无食物。拉替拉韦对肝细胞色素 P450 活性有一周的影响(抑制或诱导)。在肾功能不全或轻至中度肝损伤时不需要调整剂量。挽救治疗领域的新范例是使几乎所有患者的病毒载量低于检测下限。很快就明显看出,这在 70-90%以上的患者中是可行的。拉替拉韦在这一新范例中被证明是关键的。拉替拉韦与优化背景治疗的安慰剂在 005 期和 BENCHMRK 研究(018 和 019)中都被用于挽救治疗。在所有三项研究中,与安慰剂相比,在 24、48 和 96 周时均显示出优越性。耐受性非常好,病毒学失败通常与整合酶基因突变的选择有关,随后是 Y143C/H/R、Q148H/K/R 或较少见的 NI55H 途径。最后,在两项 SWITCHMRK 研究中,在接受含有洛匹那韦/利托那韦的稳定 cART 治疗且病毒学抑制的患者中,拉替拉韦与洛匹那韦/利托那韦相比不能证明非劣效性。最可能的解释是存在对背景治疗的存档耐药突变,导致拉替拉韦的功能单药治疗。